Impact of Lung Compliance on Neurological Outcome in Patients with Acute Respiratory Distress Syndrome Following Out-of-Hospital Cardiac Arrest


Abstract
:1. Introduction
2. Materials and Methods
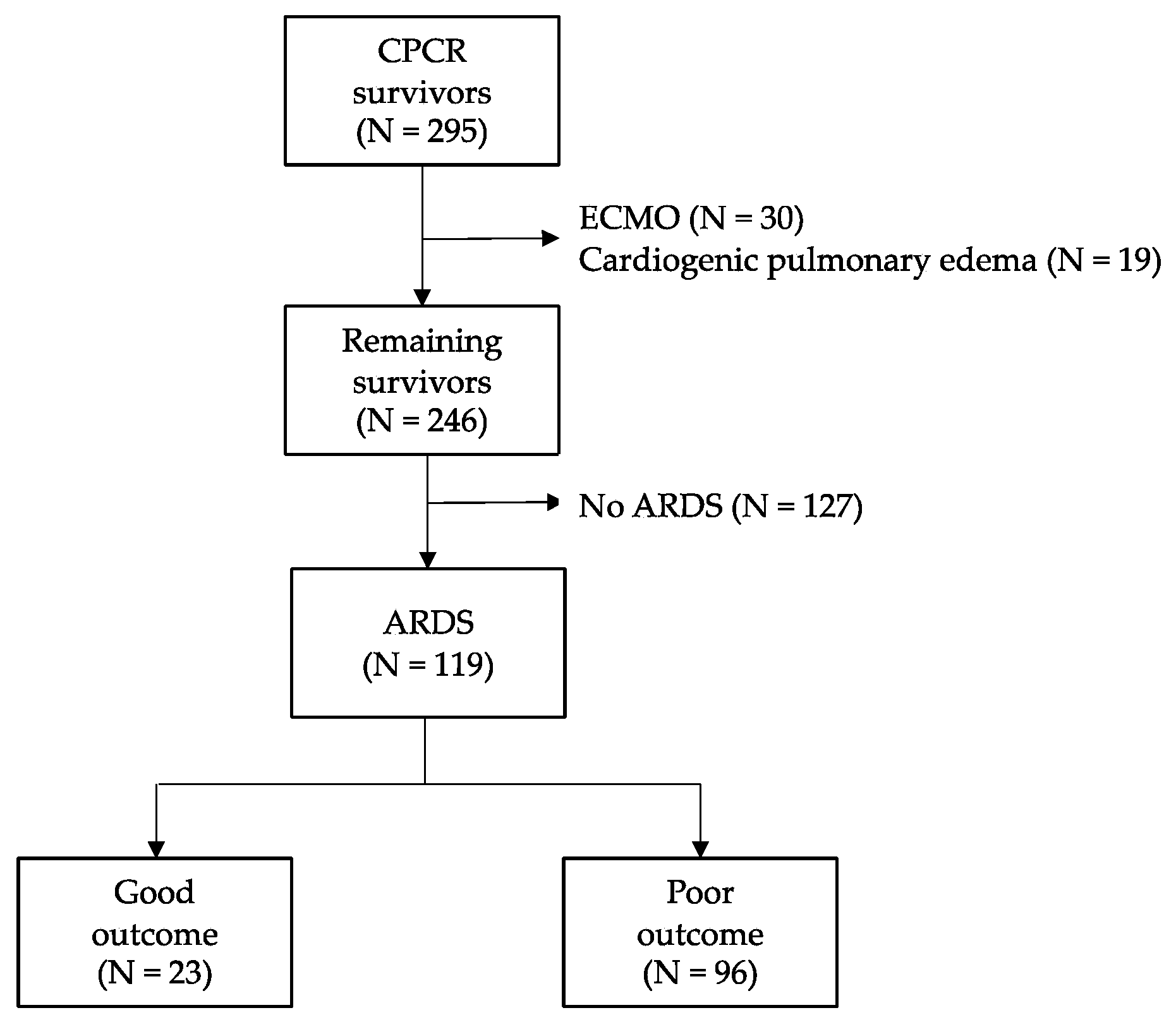
2.1. Study Design and Population
2.2. Routine Post-Cardiac Arrest Care Protocol
2.3. Definition of Variables
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Mechanical Ventilator Parameters on Admission and Neurologic Outcome
3.3. Compliance and Good Neurologic Outcome
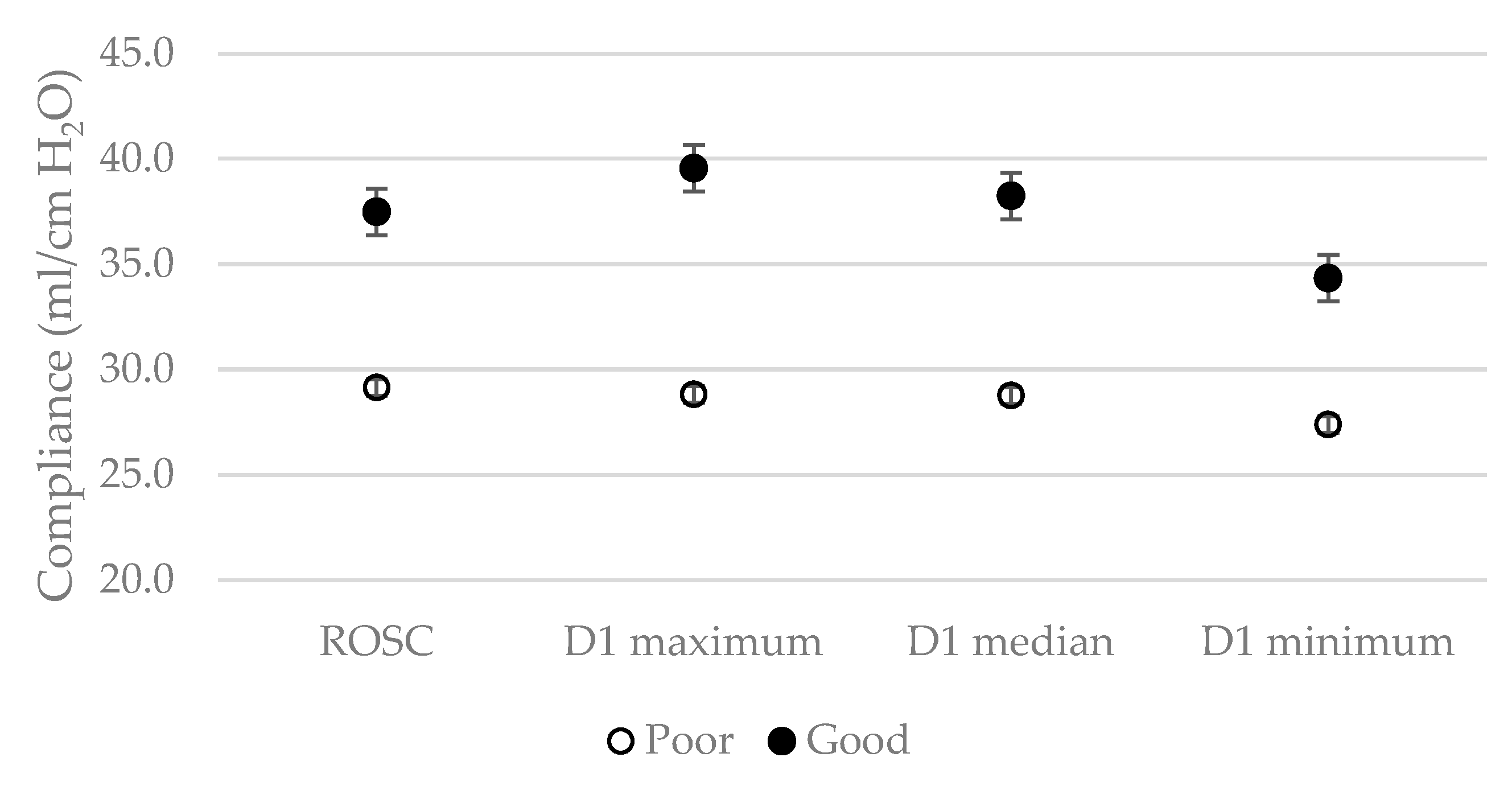
3.4. Differences of Day-1 Compliance for Neurologic Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.W.; Holmberg, M.J.; Berg, K.M.; Donnino, M.W.; Granfeldt, A. In-hospital cardiac arrest. JAMA 2019, 321, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Myat, A.; Song, K.-J.; Rea, T. Out-of-hospital cardiac arrest: Current concepts. Lancet 2018, 391, 970–979. [Google Scholar] [CrossRef]
- Stub, D.; Bernard, S.; Duffy, S.J.; Kaye, D.M. Post cardiac arrest syndrome. Circulation 2011, 123, 1428–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, N.J.; Caldwell, E.; Carlbom, D.J.; Gaieski, D.F.; Prekker, M.E.; Rea, T.D.; Sayre, M.; Hough, C.L. The acute respiratory distress syndrome after out-of-hospital cardiac arrest: Incidence, risk factors, and outcomes. Resuscitation 2019, 135, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Pierrakos, C.; Karanikolas, M.; Scolletta, S.; Karamouzos, V.; Velissaris, D. Acute respiratory distress syndrome: Pathophysiology and therapeutic options. J. Clin. Med. Res. 2012, 4, 7. [Google Scholar]
- Harmon, M.; van Meenen, D.M.; van der Veen, A.L.; Binnekade, J.M.; Dankiewicz, J.; Ebner, F.; Nielsen, N.; Pelosi, P.; Schultz, M.J.; Horn, J.; et al. Practice of mechanical ventilation in cardiac arrest patients and effects of targeted temperature management: A sub study of the targeted temperature management trial. Resuscitation 2018, 129, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Sutherasan, Y.; Peñuelas, O.; Muriel, A.; Vargas, M.; Frutos-Vivar, F.; Brunetti, I.; Raymondos, K.; D’Antini, D.; Nielsen, N.; Ferguson, N.D.; et al. Management and outcome of mechanically ventilated patients after cardiac arrest. Crit. Care 2015, 19, 215. [Google Scholar] [CrossRef] [Green Version]
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute respiratory distress syndrome. JAMA 2018, 319, 698–710. [Google Scholar] [CrossRef]
- Fan, E.; Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.; Amato, M.B.; Branson, R.; Brower, R.G.; et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef]
- Mai, N.; Rhodes, K.M.; Knowlden, S.; Halterman, M.W. The post-cardiac arrest syndrome: A case for lung-brain coupling and opportunities for neuroprotection. J. Cereb. Blood Flow. Metab. 2019, 39, 939–958. [Google Scholar] [CrossRef]
- Henderson, W.R.; Chen, L.; Amato, M.B.; Brochard, L.J. Fifty years of research in ARDS. Respiratory mechanics in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2017, 196, 822–833. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, S.M.; Jeon, S.-B.; Sohn, C.H.; Ahn, S.; Han, C.; Lee, B.K.; Lee, D.H.; Kim, S.H.; Donnino, M.W.; Kim, W.Y. Predicting outcome with diffusion-weighted imaging in cardiac arrest patients receiving hypothermia therapy. Crit. Care Med. 2015, 43, 2370–2377. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Ahn, S.; Sohn, C.H.; Seo, D.-W.; Lee, Y.-S.; Lee, J.H.; Oh, B.J.; Lim, K.S.; Kim, W.Y. Long-term neurological outcomes in patients after out-of-hospital cardiac arrest. Resuscitation 2016, 101, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-J.; Kim, Y.H.; Lee, B.K.; Park, Y.S.; Sim, M.S.; Kim, S.J.; Oh, S.H.; Lee, D.H.; Kim, W.Y. Immediate versus early coronary angiography with targeted temperature management in out-of-hospital cardiac arrest survivors without ST-segment elevation: A propensity score-matched analysis from a multicenter registry. Resuscitation 2019, 135, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Elmer, J. Exposure to high concentrations of inspired oxygen does not worsen lung injury after cardiac arrest. Crit. Care 2015, 19, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girardis, M.; Busani, S.; Damiani, E.; Donati, A.; Rinaldi, L.; Marudi, A.; Morelli, A.; Antonelli, M.; Singer, M. Effect of conservative vs conventional oxygen therapy on mortality among patients in an intensive care unit: The oxygen-ICU randomized clinical trial. JAMA 2016, 316, 1583–1589. [Google Scholar] [CrossRef]
- Cha, K.C.; Kim, Y.W.; Kim, H.I.; Kim, O.H.; Cha, Y.S.; Kim, H.; Lee, K.H.; Hwang, S.O. Parenchymal lung injuries related to standard cardiopulmonary resuscitation. Am. J. Emerg. Med. 2017, 35, 117–121. [Google Scholar] [CrossRef]
- Ruemmler, R.; Ziebart, A.; Moellmann, C.; Garcia-Bardon, A.; Kamuf, J.; Kuropka, F.; Duenges, B.; Hartmann, E. Ultra-low tidal volume ventilation—A novel and effective ventilation strategy during experimental cardiopulmonary resuscitation. Resuscitation 2018, 132, 56–62. [Google Scholar] [CrossRef]
- Eastwood, G.M.; Tanaka, A.; Espinoza, E.; Peck, L.; Young, H.; Mårtensson, J.; Zhang, L.; Glassford, N.J.; Hsiao, Y.-F.; Suzuki, S.; et al. Conservative oxygen therapy in mechanically ventilated patients following cardiac arrest: A retrospective nested cohort study. Resuscitation 2016, 101, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Gajic, O.; Dara, S.I.; Mendez, J.L.; Adesanya, A.O.; Festic, E.; Caples, S.M.; Rana, R.; Sauver, J.L.; Lymp, J.F.; Afessa, B.; et al. Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation. Crit. Care Med. 2004, 32, 1817–1824. [Google Scholar] [CrossRef] [PubMed]
- Neto, A.; Nagtzaam, L.; Schultz, M.J. Ventilation with lower tidal volumes for critically ill patients without the acute respiratory distress syndrome. Curr. Opin. Crit. Care 2014, 20, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Forel, J.-M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.-M.; Perez, D.; Seghboyan, J.-M.; et al. Neuromuscular blockers in early acute respiratory distress syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Kilgannon, J.H.; Jones, A.E.; Parrillo, J.E.; Dellinger, R.P.; Milcarek, B.; Hunter, K.; Shapiro, N.I.; Trzeciak, S. for Emergency Medicine Shock Research Network (EMShockNet) Investigators. Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation 2011, 123, 2717–2722. [Google Scholar] [CrossRef] [Green Version]
- Jakkula, P.; Reinikainen, M.; Hästbacka, J.; Loisa, P.; Tiainen, M.; Pettilä, V.; Toppila, J.; Lähde, M.; Bäcklund, M.; Okkonen, M.; et al. Targeting two different levels of both arterial carbon dioxide and arterial oxygen after cardiac arrest and resuscitation: A randomized pilot trial. Intensive Care Med. 2018, 44, 2112–2121. [Google Scholar] [CrossRef] [Green Version]
- Nolan, J.P.; Soar, J.; Cariou, A.; Croberg, T.; Moulaert, V.R.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunda, K.; Sandroni, C. European resuscitation council and European society of intensive care medicine guidelines for post-resuscitation care 2015 section 5 of the European, resuscitation council guidelines for resuscitation 2015. Resuscitation 2015, 95, 202–222. [Google Scholar] [CrossRef]
- Che, D.; Li, L.; Kopil, C.M.; Liu, Z.; Guo, W.; Neumar, R.W. Impact of therapeutic hypothermia onset and duration on survival, neurologic function, and neurodegeneration after cardiac arrest. Crit. Care Med. 2011, 39, 1423–1430. [Google Scholar] [CrossRef] [Green Version]
- Horn, M.; Schlote, W. Delayed neuronal death and delayed neuronal recovery in the human brain following global ischemia. Acta Neuropathol. 1992, 85, 79–87. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total (n = 119) | Poor Outcome (n = 96) | Good Outcome (n = 23) | p-Value |
|---|---|---|---|---|
| Age | 67.0 (57.0–78.0) | 69.0 (61.0–77.0) | 62.0 (52.0–80.5) | 0.770 |
| Male | 76 (63.9) | 59 (61.5) | 17 (73.9) | 0.264 |
| BMI (kg/m2) | 23.7 (21.1–26.1) | 22.9 (20.8–26.0) | 23.3 (18.9–26.2) | 0.719 |
| Smoker | 44 (37.0) | 33 (34.4) | 11 (47.8) | 0.235 |
| Past history | ||||
| Previous ACS | 21 (17.6) | 16 (16.7) | 5 (21.7) | 0.567 |
| Previous PCI | 15 (12.6) | 11 (11.5) | 4 (17.4) | 0.441 |
| Hypertension | 58 (48.7) | 50 (52.1) | 8 (34.8) | 0.136 |
| Diabetes mellitus | 44 (37.0) | 38 (39.6) | 6 (26.1) | 0.228 |
| COPD | 12 (10.1%) | 12 (12.5) | 0 (0.0) | 0.075 |
| CKD | 23 (19.3) | 20 (20.8) | 3 (13.0) | 0.560 |
| Malignancy | 14 (11.8) | 12 (12.5) | 2 (8.7) | 0.599 |
| Characteristics of Cardiac arrest | ||||
| Witnessed arrest | 83 (69.7) | 65 (67.7) | 18 (78.3) | 0.324 |
| Bystander CPR | 78 (65.5) | 63 (65.6) | 15 (65.2) | 0.814 |
| Shockable rhythm | 22 (23.2) | 13 (16.0) | 9 (64.3) | <0.001 |
| Cardiac caused | 51 (42.9) | 36 (37.5) | 15 (65.2) | 0.016 |
| Time of CA to resuscitation (min) | 5.0 (0.0–9.0) | 5.0 (0.0–9.0) | 4.0 (0.0–6.5) | 0.708 |
| Total CPR time (min) | 29.0 (15.0–41.0) | 31.5 (21.3–43.8) | 11.0 (4.0–21.0) | <0.001 |
| ARDS risk factors | ||||
| Shock | 69 (58.0) | 62 (64.6) | 7 (30.4) | 0.003 |
| Aspiration | 62 (52.1) | 51 (53.1) | 11 (47.8) | 0.648 |
| Pancreatitis | 3 (2.5) | 3 (3.1) | 0 (0.0) | 0.253 |
| Pneumonia | 44 (37.0) | 36 (37.5) | 8 (34.8) | 0.808 |
| Pulmonary contusion | 85 (71.4) | 69 (71.9) | 16 (69.6) | 0.827 |
| Sepsis, no pneumonia | 19 (16.0) | 16 (16.7) | 3 (13.0) | 0.664 |
| Sedative and NMB during TTM | ||||
| Midazolam | 26 (21.8) | 22 (22.9) | 4 (17.4) | 0.565 |
| Ketamine | 2 (1.7) | 2 (2.1) | 0 (0.0) | 0.352 |
| Morphine | 38 (31.9) | 31 (32.3) | 7 (30.4) | 0.863 |
| Propofol | 80 (67.2) | 59 (61.5) | 21 (91.3) | 0.003 |
| Fentanyl | 58 (48.7) | 45 (46.9) | 13 (56.5) | 0.405 |
| Continuous NMB | 54 (45.4) | 42 (43.8) | 12 (52.2) | 0.467 |
| ICU care factors | ||||
| BT, before TTM applied (°C) | 35.9 (35.1–36.5) | 35.8 (35.0–36.5) | 35.8 (35.2–36.2) | 0.521 |
| Lactate, after ROSC (mmol/L) | 12.7 (9.4–15.0) | 13.2 (10.1–15.0) | 9.3 (6.4–13.0) | 0.002 |
| Acquired pneumonia | 12 (10.1) | 7 (7.3) | 5 (21.7) | 0.040 |
| Acquired UTI | 2 (1.7) | 2 (2.1) | 0 (0.0) | 0.485 |
| SOFA at admission | 12.0 (11.0–15.0) | 12.0 (11.0–15.0) | 11.5 (10.5–15.0) | 0.654 |
| MV duration (day) | 7.0 (3.0–9.0) | 7.0 (2.0–9.0) | 7.0 (5.0–13.0) | 0.050 |
| Parameters | Total (n = 119) | Poor Outcome (n = 96) | Good Outcome (n = 23) | p-Value |
|---|---|---|---|---|
| pH | 7.0 (6.9–7.2) | 7.0 (6.8–7.2) | 7.2 (7.0–7.3) | 0.001 |
| FiO2 (%) | 100.0 (80.0–100.0) | 100.0 (90.0–100.0) | 100.0 (60.0–100.0) | 0.028 |
| PaO2 (mmHg) | 86.0 (68.4–115.8) | 86.0 (70.4–115.8) | 77.1 (62.5–137.4) | 0.287 |
| PaCO2 (mmHg) | 54.0 (40.0–73.0) | 57.0 (43.5–76.0) | 46.0 (32.6–60.5) | 0.005 |
| PEEP (cm H2O) | 5.0 (4.0–8.0) | 5.0 (4.0–8.0) | 5.0 (4.0–7.0) | 0.638 |
| Inspiratory pressure (cm H2O) | 15.0 (12.0–18.0) | 16.0 (14.0–18.0) | 12.0 (12.0–13.5) | <0.001 |
| Pplat (cm H2O) | 21.0 (17.3–25.8) | 21.0 (18.0–22.0) | 17.0 (16.0–20.0) | <0.001 |
| Respiratory rate | 20.0 (18.0–22.0) | 20.0 (18.0–22.0) | 18.0 (15.0–20.0) | 0.013 |
| Tidal volume (mL) | 427.0 (367.0–497.0) | 420.0 (360.0–489.5) | 458.0 (395.5–545.0) | 0.053 |
| Compliance (ml/cm H2O) | 29.7 (21.8–36.9) | 27.5 (21.6–34.0) | 38.6 (33.1–46.2) | <0.001 |
| Minute ventilation (L/min) | 8.2 (7.6–10.4) | 8.8 (7.7–10.3) | 8.8 (6.5–10.7) | 0.609 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | Adjusted HR | 95% CI | p-Value | |
| Shockable | 1.47 | 1.22–1.77 | <0.001 | 1.28 | 1.01–1.63 | 0.039 |
| Cardiac cause | 2.10 | 0.92–4.82 | 0.080 | 1.99 | 0.55–7.23 | 0.293 |
| Carbon dioxide | 0.97 | 0.94–0.99 | 0.017 | 0.99 | 0.96–1.02 | 0.643 |
| CPR duration | 0.96 | 0.93–1.00 | 0.060 | 0.94 | 0.90–1.00 | 0.038 |
| Compliance | ||||||
| Maximum | 1.03 | 1.01–1.05 | <0.001 | 1.05 | 1.02–1.09 | <0.001 |
| Minimum | 1.04 | 1.02–1.06 | <0.001 | 1.08 | 1.03–1.13 | <0.001 |
| Median | 1.04 | 1.02–1.06 | <0.001 | 1.06 | 1.02–1.09 | <0.001 |
| Sensitivity | Specificity | PLR | NLR | PPV | NPV | |
|---|---|---|---|---|---|---|
| D1 max >32.5 | 69.5 | 72.0 | 2.48 | 0.42 | 90.4 | 38.3 |
| D1 min >28.6 | 64.9 | 66.7 | 1.95 | 0.53 | 88.4 | 32.7 |
| D1 median >31.4 | 59.3 | 66.7 | 1.78 | 0.61 | 90.0 | 24.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-s.; Kim, Y.-J.; Kim, M.; Ryoo, S.M.; Sohn, C.H.; Ahn, S.; Kim, W.Y. Impact of Lung Compliance on Neurological Outcome in Patients with Acute Respiratory Distress Syndrome Following Out-of-Hospital Cardiac Arrest. J. Clin. Med. 2020, 9, 527. https://doi.org/10.3390/jcm9020527
Kim J-s, Kim Y-J, Kim M, Ryoo SM, Sohn CH, Ahn S, Kim WY. Impact of Lung Compliance on Neurological Outcome in Patients with Acute Respiratory Distress Syndrome Following Out-of-Hospital Cardiac Arrest. Journal of Clinical Medicine. 2020; 9(2):527. https://doi.org/10.3390/jcm9020527
Chicago/Turabian StyleKim, June-sung, Youn-Jung Kim, Muyeol Kim, Seung Mok Ryoo, Chang Hwan Sohn, Shin Ahn, and Won Young Kim. 2020. "Impact of Lung Compliance on Neurological Outcome in Patients with Acute Respiratory Distress Syndrome Following Out-of-Hospital Cardiac Arrest" Journal of Clinical Medicine 9, no. 2: 527. https://doi.org/10.3390/jcm9020527