Selective ß2-Adrenoceptor Agonists and Relevant Hyperlactatemia: Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Literature Search Strategy
2.2. Selection Criteria and Data Extraction
2.3. Study Quality Assessment
3. Analysis
4. Results
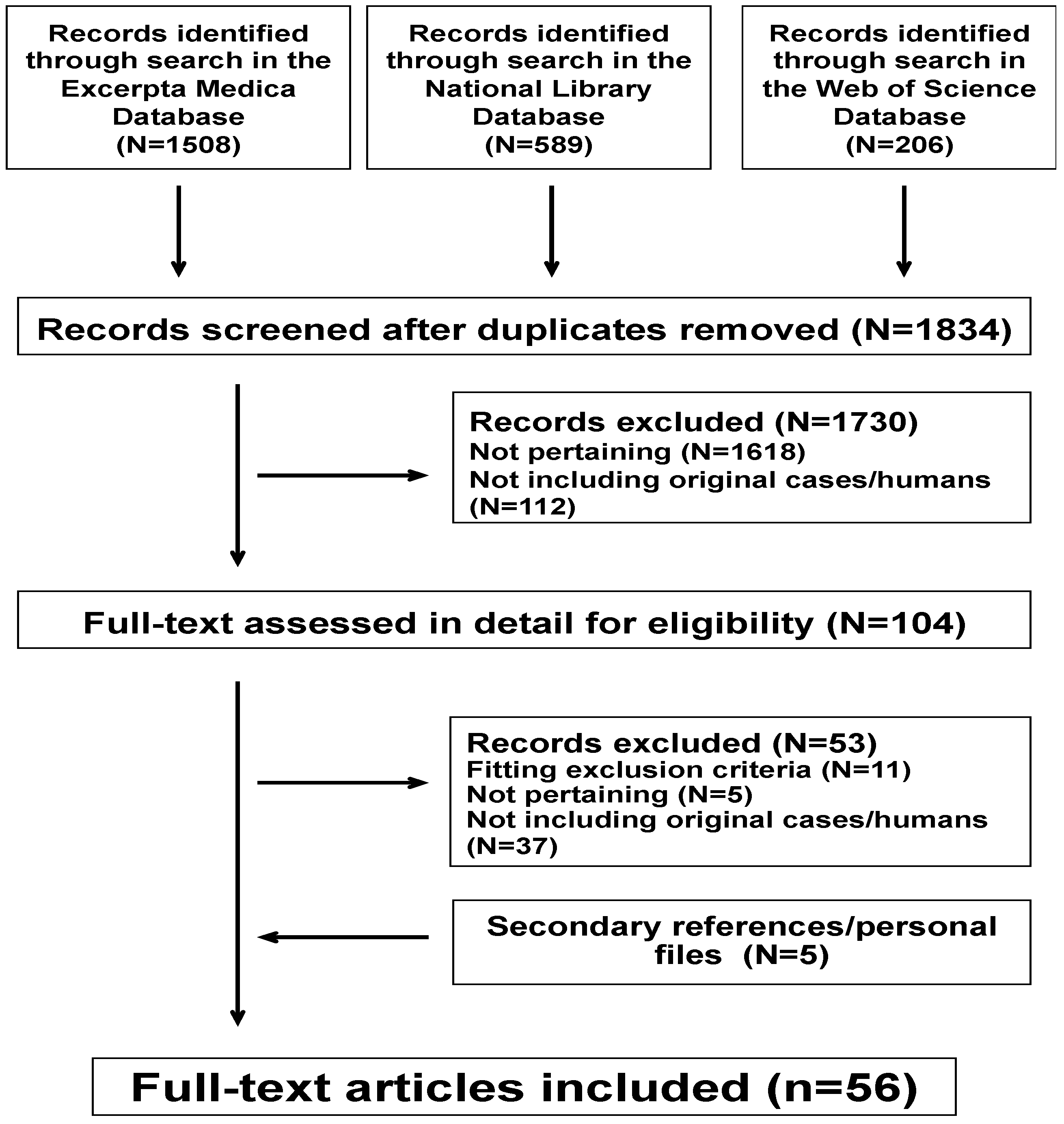
4.1. Literature Search Results
4.2. Individual Cases
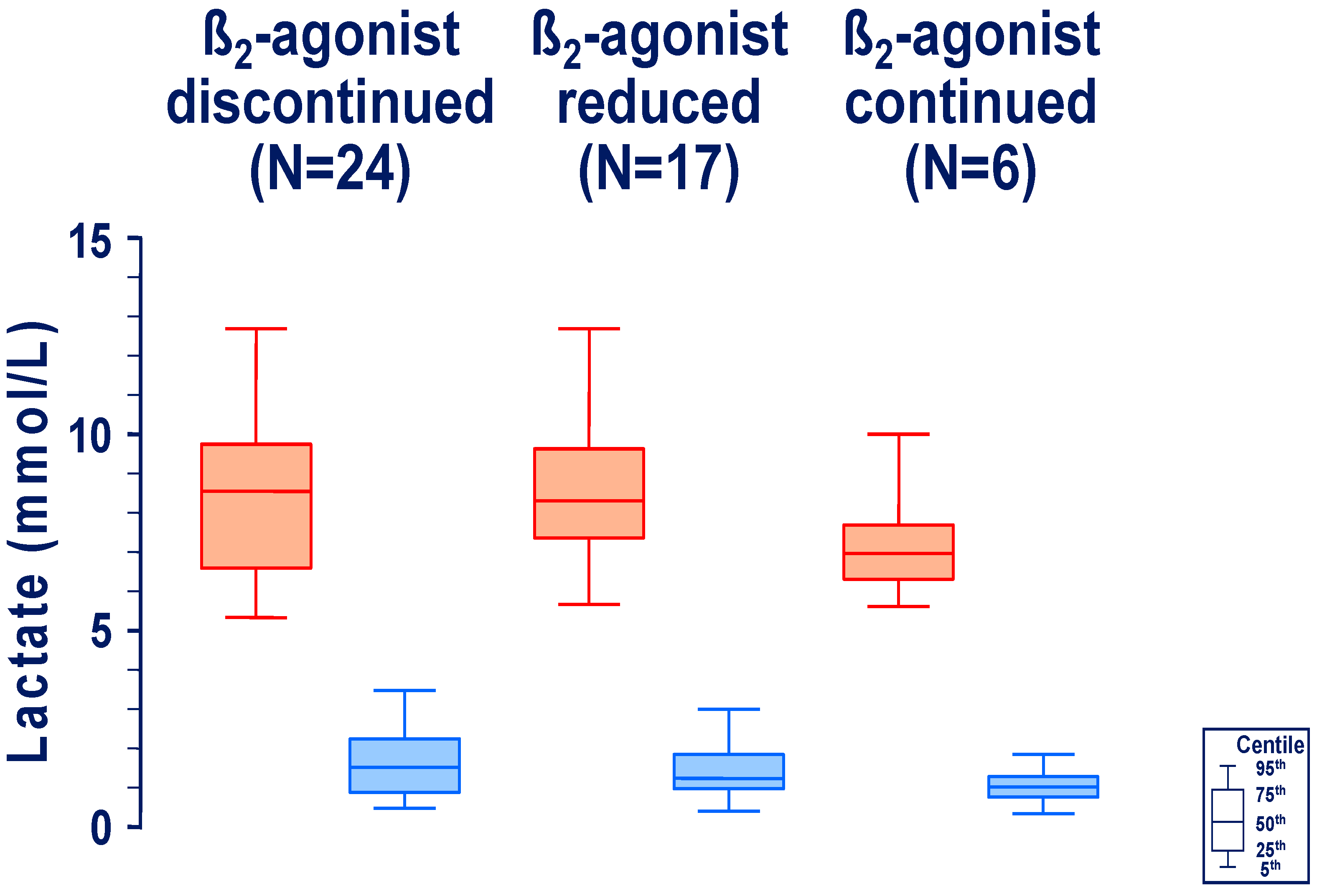
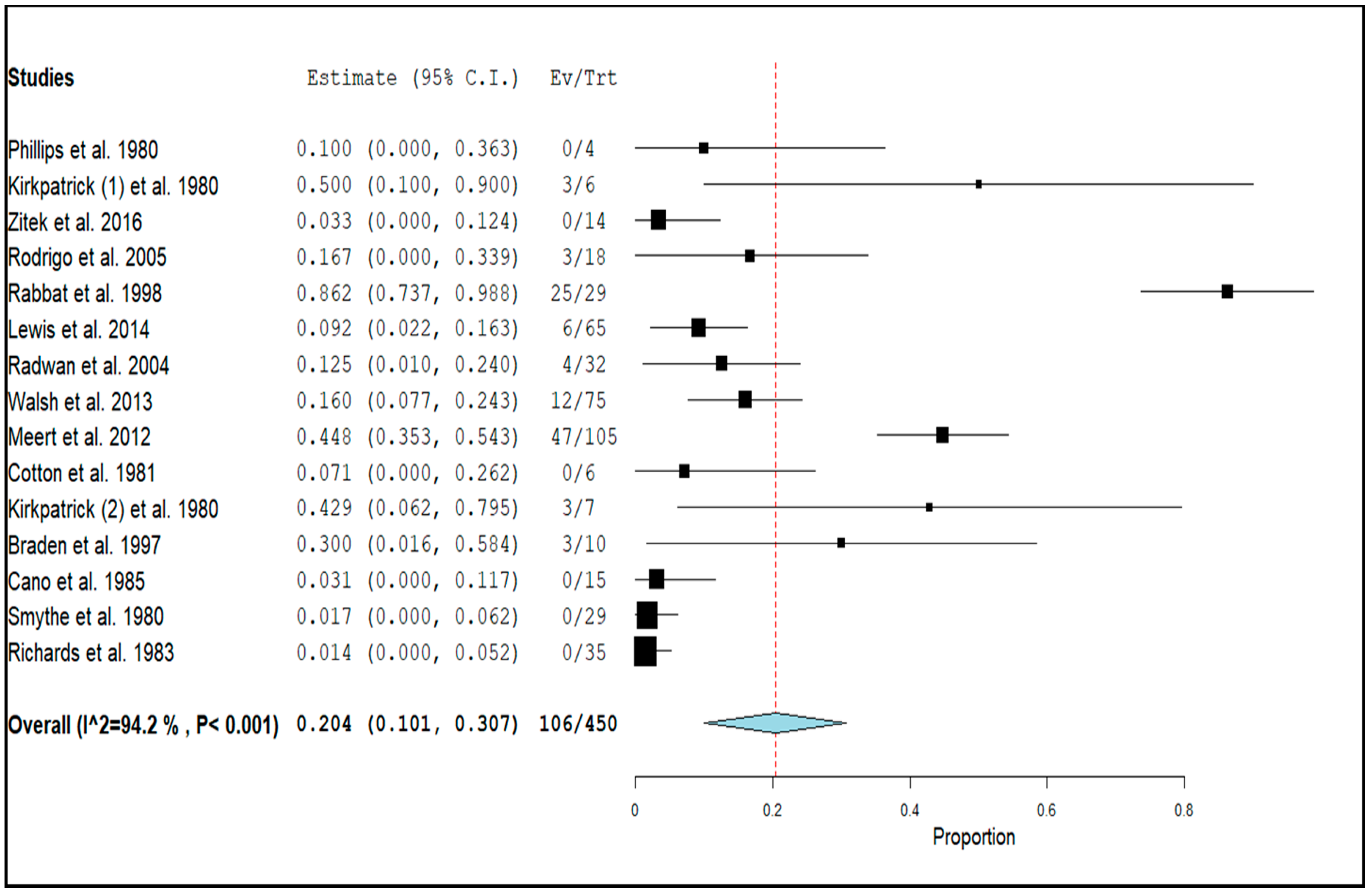
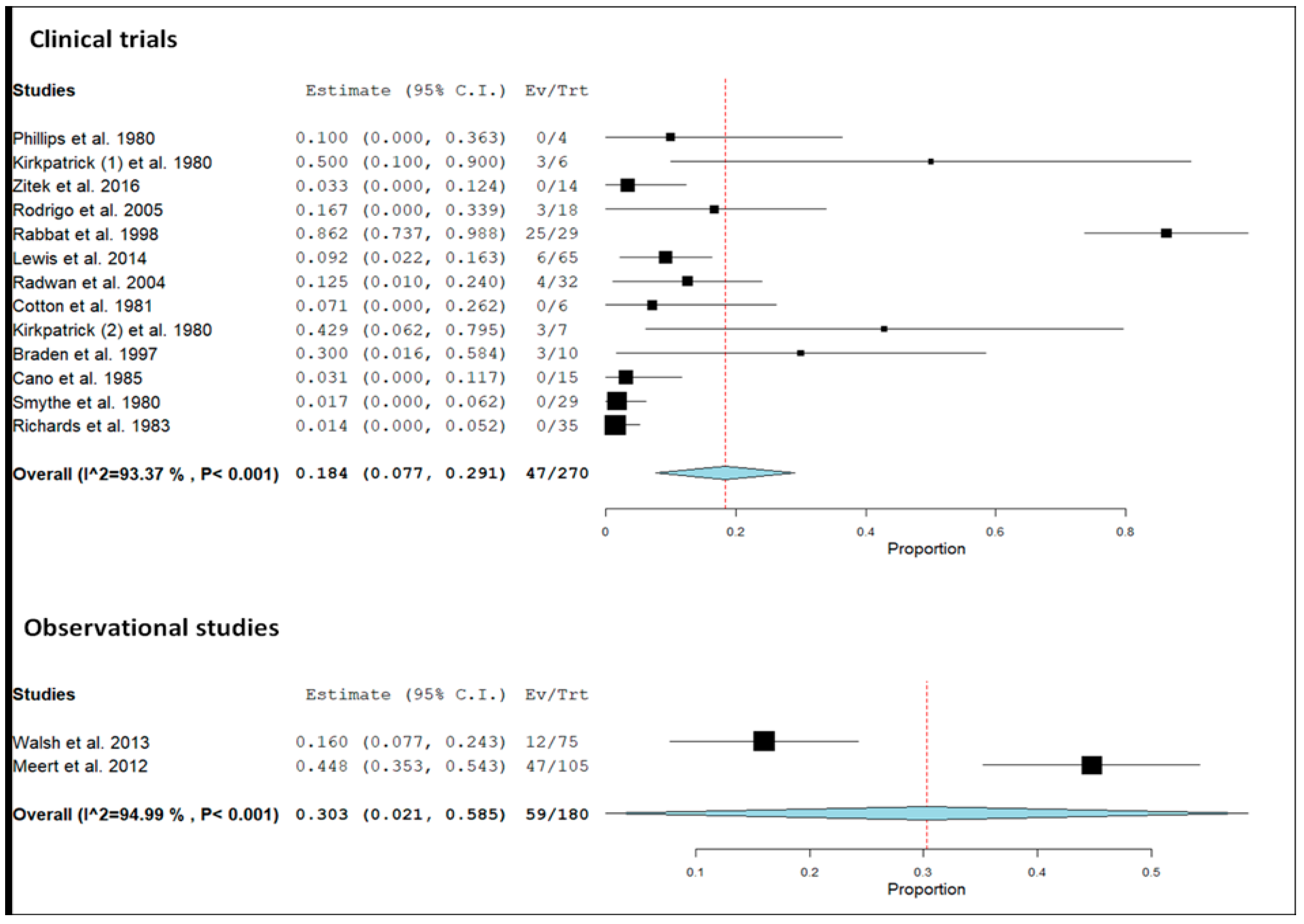
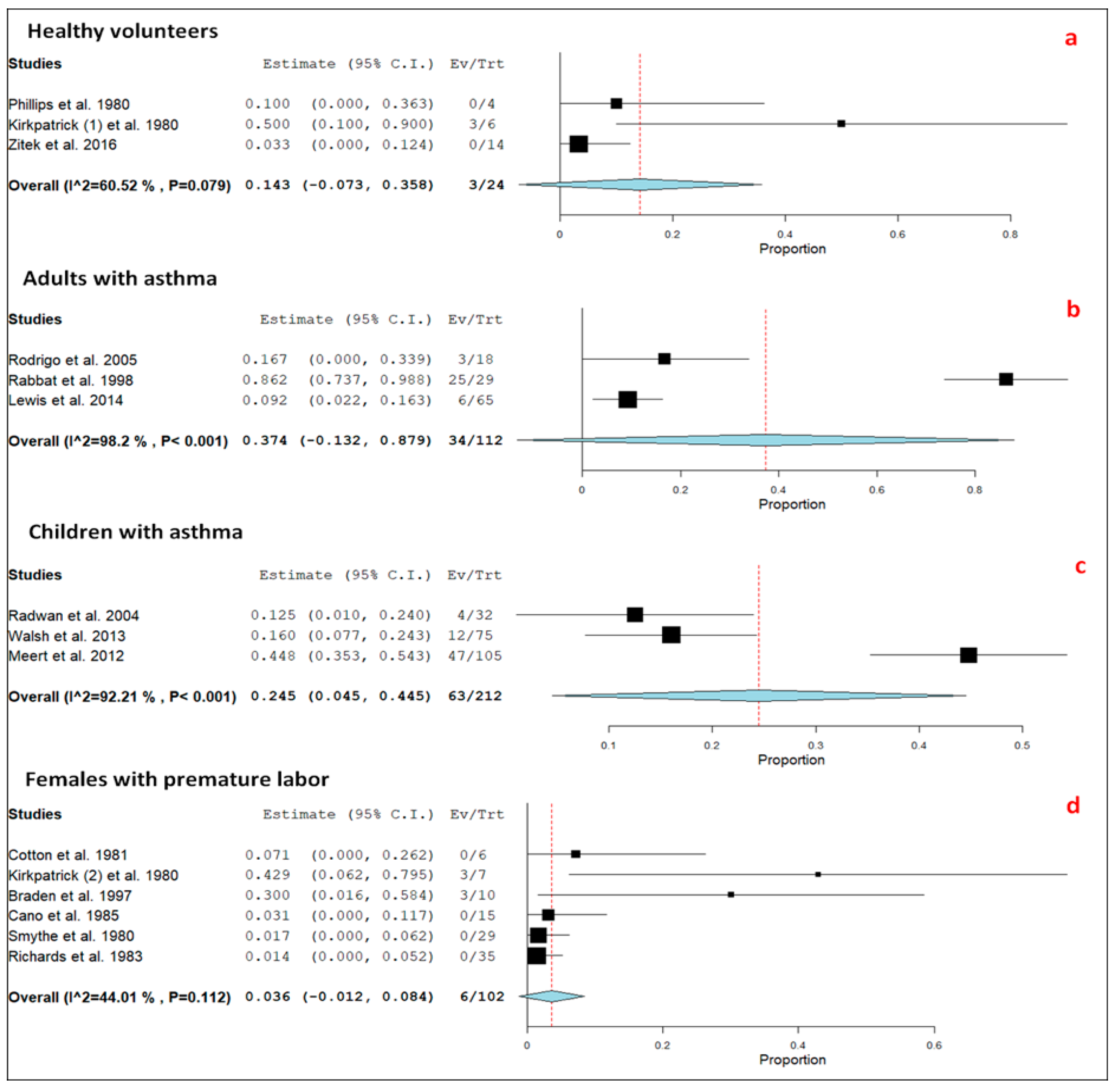
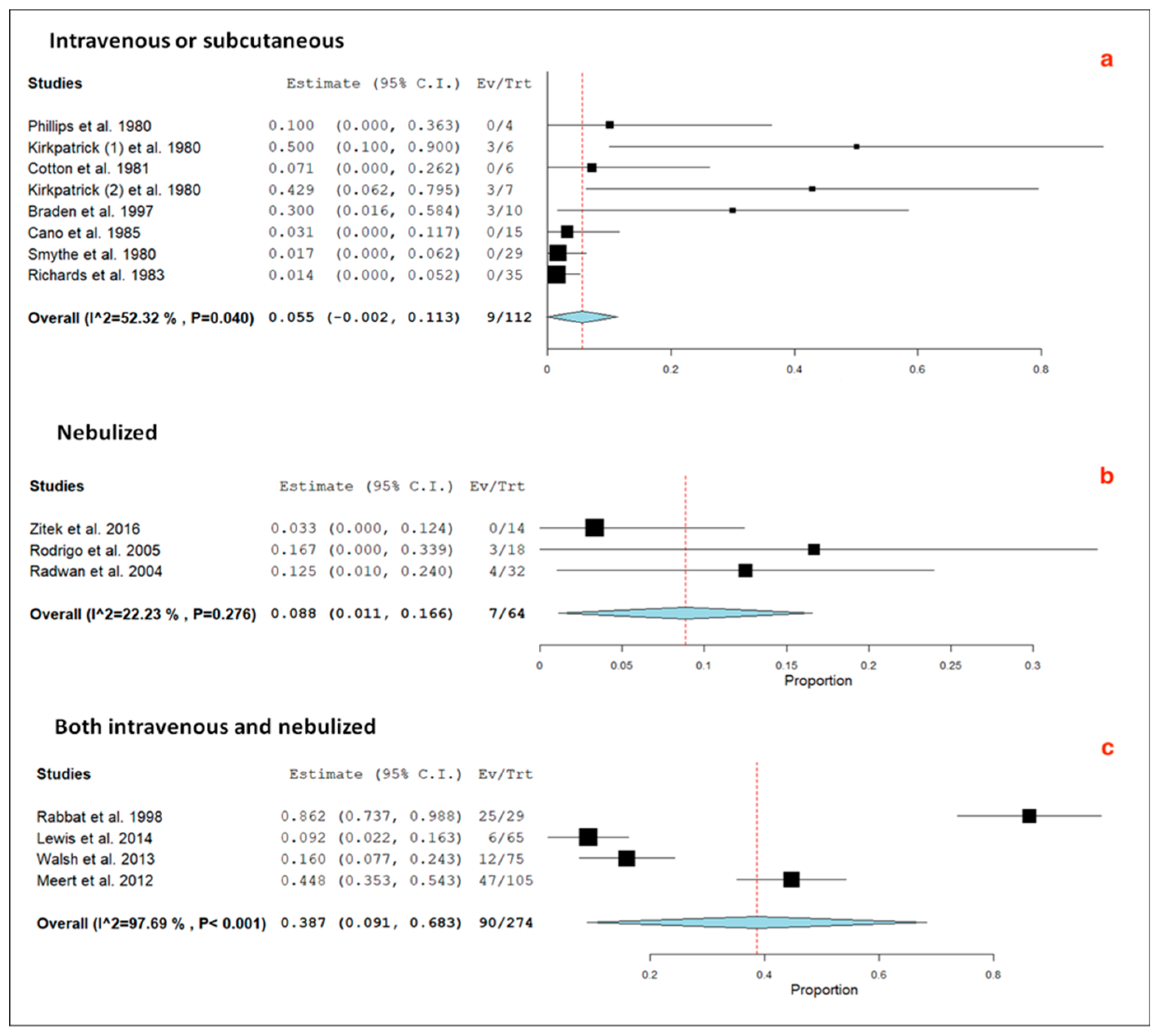
4.3. Observational Studies and Clinical Trials
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Reddy, A.J.; Lam, S.W.; Bauer, S.R.; Guzman, J.A. Lactic acidosis: Clinical implications and management strategies. Cleve. Clin. J. Med. 2015, 82, 615–624. [Google Scholar] [CrossRef]
- Smith, Z.R.; Horng, M.; Rech, M.A. Medication-induced hyperlactatemia and lactic acidosis: A systematic review of the literature. Pharmacotherapy 2019, 39, 946–963. [Google Scholar] [CrossRef]
- Levy, B.; Desebbe, O.; Montemont, C.; Gibot, S. Increased aerobic glycolysis through ß2 stimulation is a common mechanism involved in lactate formation during shock states. Shock 2008, 30, 417–421. [Google Scholar] [CrossRef]
- Désir, D.; Van Coevorden, A.; Kirkpatrick, C.; Caufriez, A. Ritodrine-induced acidosis in pregnancy. Br. Med. J. 1978, 277, 1194. [Google Scholar] [CrossRef] [Green Version]
- Israel, E.; Reddel, H.K. Severe and difficult-to-treat asthma in adults. N. Engl. J. Med. 2017, 377, 965–976. [Google Scholar] [CrossRef]
- Rundell, K.; Panchal, B. Preterm labor: Prevention and management. Am. Fam. Physician 2017, 95, 366–372. [Google Scholar] [PubMed]
- Mirza, S.; Clay, R.D.; Koslow, M.A.; Scanlon, P.D. COPD Guidelines: A review of the 2018 GOLD Report. Mayo Clin. Proc. 2018, 93, 1488–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braden, G.L.; Johnston, S.S.; Germain, M.J.; Fitzgibbons, J.P.; Dawson, J.A. Lactic acidosis associated with the therapy of acute bronchospasm. N. Engl. J. Med. 1985, 313, 890–891. [Google Scholar] [CrossRef] [PubMed]
- Saint-Jean, O.; de Rohan Chabot, P.; Thaler, F.; Loirat, P. Hyperlactatémie lors du traitement d’un bronchospasme aigu avec du salbutamol. Presse Méd. 1987, 16, 965–966. [Google Scholar]
- Assadi, F.K. Therapy of Acute Bronchospasm: Complicated by Lactic Acidosis and Hypokalemia. Clin. Pediatr. 1989, 28, 258–260. [Google Scholar] [CrossRef]
- Maury, E.; Ioos, V.; Lepecq, B.; Guidet, B.; Offenstadt, G. A paradoxical effect of bronchodilators. Chest 1997, 111, 1766–1777. [Google Scholar] [CrossRef] [PubMed]
- Manthous, C.A. Lactic acidosis in status asthmaticus: Three cases and review of the literature. Chest 2001, 119, 1599–1602. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Mehta, S. Lactic acidosis in asthma: Report of two cases and review of the literature. Can. Respir. J. 2002, 9, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Liem, E.B.; Mnookin, S.C.; Mahla, M.E. Albuterol-induced lactic acidosis. Anesthesiology 2003, 99, 505–506. [Google Scholar] [CrossRef]
- Du-Thanh, A.; Groleron, S.; Le Quellec, A. Acidose lactique sous β2 mimétiques inhalés et asthme: À propos d’un cas et revue de la littérature. Rev. Med. Interne 2004, 25, 470–471. [Google Scholar] [CrossRef]
- Girgis, M.; Milner, Q. A rare side-effect of intravenous salbutamol. Anaesthesia 2004, 59, 196–197. [Google Scholar] [CrossRef]
- Sobolev, I. A response to ‘A rare side-effect of intravenous salbutamol’, Girgis M and Milner, Q. Anaesthesia 2004, 59, 730. [Google Scholar] [CrossRef]
- Tobin, A.; Santamaria, J. Respiratory failure precipitated by salbutamol. J. Intern. Med. 2005, 35, 199–200. [Google Scholar] [CrossRef]
- Fekih-Hassen, M.; Ayed, S.; Brahem, H.; Marghili, S.; Elatrous, S. Acidose lactique induite par la terbutaline au cours de l’asthme aigu grave. Rev. Pneumol. Clin. 2006, 62, 203–204. [Google Scholar] [CrossRef]
- Chaulier, K.; Chalumeau, S.; Ber, C.E.; Bret, M.; Rimmelé, T. Acidose métabolique dans un contexte d’asthme aigu grave. Ann. Fr. Anesth. Réanim. 2007, 26, 352–355. [Google Scholar] [CrossRef]
- Jee, R.; Brownlow, H. Hyperlactaemia due to nebulised salbutamol. Anaesthesia 2007, 62, 751–752. [Google Scholar] [CrossRef] [PubMed]
- Koul, P.B.; Minarik, M.; Totapally, B.R. Lactic acidosis in children with acute exacerbation of severe asthma. Eur. J. Emerg. Med. 2007, 14, 56–58. [Google Scholar] [CrossRef]
- Meert, K.L.; Clark, J.; Sarnaik, A.P. Metabolic acidosis as an underlying mechanism of respiratory distress in children with severe acute asthma. Pediatr. Crit. Care Med. 2007, 8, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Gómez Bustos, M.D.; García Ron, A.; Ibarra de la Rosa, I.; Pérez Navero, J.L. Acidosis láctica secundaria a inhalación de dosis elevadas de salbutamol. Pediatrics 2008, 69, 586–587. [Google Scholar] [CrossRef]
- Veenith, T.V.; Pearce, A. A case of lactic acidosis complicating assessment and management of asthma. Int. Arch. Med. 2008, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- González Jiménez, D.; Concha Torre, A.; Menéndez Cuervo, S.; García Hernández, I. Acidosis láctica por salbutamol en un niño con crisis asmática grave. Pediatrics 2009, 71, 82–83. [Google Scholar] [CrossRef]
- Kovacevic, A.; Schwahn, B.; Schuster, A. Hyperlactic acidosis as metabolic side-effect of albuterol and theophylline in acute severe asthma. Klin. Pädiatr. 2010, 222, 271–272. [Google Scholar] [CrossRef] [PubMed]
- Saxena, R.; Marais, G. Salbutamol: Beware of the paradox! BMJ Case Rep. 2010, 2010, bcr0120102665. [Google Scholar] [CrossRef] [Green Version]
- Ganaie, M.B.; Hughes, R. An unusual case of lactic acidosis. Br. J. Med. Pract. 2011, 4, a420. [Google Scholar]
- McGonigle, R.; Woods, R.A. Take my breath away: A case of lactic acidosis in an asthma exacerbation. CJEM 2011, 13, 284–288. [Google Scholar] [CrossRef] [Green Version]
- Berman, S.B.; Liao, J.S. Albuterol-induced lactic acidosis: A case report. Proc. UCLA Health 2012, 16, 10–12. [Google Scholar]
- Claret, P.G.; Bobbia, X.; Boutin, C.; Rougier, M.; de la Coussaye, J.E. Lactic acidosis as a complication of β-adrenergic aerosols. Am. J. Emerg. Med. 2012, 30, 1319. [Google Scholar] [CrossRef] [PubMed]
- Dodda, V.R.; Spiro, P. Can albuterol be blamed for lactic acidosis? Respir. Care 2012, 57, 2115–2118. [Google Scholar] [CrossRef] [PubMed]
- Manara, A.; Hantson, P.; Vanpee, D.; Thys, F. Lactic acidosis following intentional overdose by inhalation of salmeterol and fluticasone. CJEM 2012, 14, 378–381. [Google Scholar] [CrossRef] [Green Version]
- Mathur, S.; Khalid, I.; Pesola, G. Beta agonist-induced lactic acidosis in asthma. Internet J. Asthma Allergy Immunol. 2012, 8, 1–3. [Google Scholar]
- Sturney, S.; Suntharalingam, J. Treating acute asthma—Salbutamol may not always be the right answer. Clin. Med. (Lond.) 2012, 12, 181–182. [Google Scholar] [CrossRef]
- Tomar, R.P.; Vasudevan, R. Metabolic acidosis due to inhaled salbutamol toxicity: A hazardous side effect complicating management of suspected cases of acute severe asthma. Med. J. Armed Forces India 2012, 68, 242–244. [Google Scholar] [CrossRef] [Green Version]
- Moustafa, F.; Garrouste, C.; Bertrand, P.M.; Kauffmann, S.; Schmidt, J. Acidose lactique post β2-mimétiques inhalés: À propos de 2 cas. Ann. Fr. Anesth. Réanim. 2014, 33, 49–51. [Google Scholar] [CrossRef]
- Perrin, C.; Savy, N.; Lang, M.; Caron, N.; Labbé, A. Acidose lactique chez un nourrisson au cours d’une crise d’asthme grave. Arch. Pédiatr. 2014, 21, 1120–1122. [Google Scholar] [CrossRef]
- Saadia, T.A.; George, M.; Lee, H. Lactic acidosis and diastolic hypotension after intermittent albuterol nebulization in a pediatric patient. Respir. Med. Case Rep. 2015, 16, 89–91. [Google Scholar] [CrossRef] [Green Version]
- Isaac, B.T.; McLellan, T.; Samuel, J.; Yung, B. Conundrum in an asthma exacerbation. BMJ Case Rep. 2016, 2016, bcr2016214360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Mondragon, A.; Delgado-García, G.; Pacheco-Cantú, A.; Contreras-Garza, N.; Galarza-Delgado, D.Á.; González-Aguirre, J. Atrial fibrillation in an asthmatic patient with albuterol-induced lactic acidosis. Pneumologia 2016, 65, 150–151. [Google Scholar] [PubMed]
- Patel, S.; Hanhan, U.; Perkowski, C.; Orlowski, J. Continuous albuterol treatments may lead to lactic acidosis in children with status asthmaticus. Int. J. Allergy Medicat. 2017, 3, 23. [Google Scholar] [CrossRef]
- Hockstein, M.; Diercks, D. Significant lactic acidosis from albuterol. Clin. Pract. Cases Emerg. Med. 2018, 2, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Sharif, Z.; Al-Alawi, M. Beware of beta! A case of salbutamol-induced lactic acidosis in severe asthma. BMJ Case Rep. 2018, 2018, bcr-2017-224090. [Google Scholar] [CrossRef]
- Martínez-Tébar, M.J.; Bodan, A.C.; García-Pachón, E. Lactic acidosis and asthma exacerbation. Arch. Bronconeumol. 2019, 55, 52. [Google Scholar] [CrossRef]
- Milani, G.P.; Lava, S.A.G.; Faré, P.B. Perla Pediatrica. Trib. Med. Tic. 2019, 84, 10–11. [Google Scholar]
- Ramakrishna, K.N.; Virk, J.; Gambhir, H.S. Albuterol-induced lactic acidosis. Am. J. Ther. 2019, 26, e635–e636. [Google Scholar] [CrossRef]
- Phillips, P.J.; Vedig, A.E.; Jones, P.L.; Chapman, M.G.; Collins, M.; Edwards, J.B.; Smeaton, T.C.; Duncan, B.M. Metabolic and cardiovascular side effects of the ß2-adrenoceptor agonists salbutamol and rimiterol. Br. J. Clin. Pharmacol. 1980, 9, 483–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zitek, T.; Cleveland, N.; Rahbar, A.; Parker, J.; Lim, C.; Elsbecker, S.; Forred, W.; Slattery, D.E. Effect of nebulized albuterol on serum lactate and potassium in healthy subjects. Acad. Emerg. Med. 2016, 23, 718–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, C.; Quenon, M.; Désir, D. Blood anions and electrolytes during ritodrine infusion in preterm labor. Am. J. Obstet. Gynecol. 1980, 138, 523–527. [Google Scholar] [CrossRef]
- Cotton, D.B.; Strassner, H.T.; Lipson, L.G.; Goldstein, D.A. The effects of terbutaline on acid base, serum electrolytes, and glucose homeostasis during the management of preterm labor. Am. J. Obstet. Gynecol. 1981, 141, 617–624. [Google Scholar] [CrossRef]
- Smythe, A.R.; Sakakini, J. Maternal metabolic alterations secondary to terbutaline therapy for premature labor. Obstet. Gynecol. 1981, 57, 566–570. [Google Scholar]
- Richards, S.R.; Chang, F.E.; Stempel, L.E. Hyperlactacidemia associated with acute ritodrine infusion. Am. J. Obstet. Gynecol. 1983, 146, 1–5. [Google Scholar] [CrossRef]
- Cano, A.; Tovar, I.; Parrilla, J.J.; Abad, L. Metabolic disturbances during intravenous use of ritodrine: Increased insulin levels and hypokalemia. Obstet. Gynecol. 1985, 65, 356–360. [Google Scholar]
- Braden, G.; von Oeyen, P.T.; Germain, M.J.; Watson, D.J.; Haag, B.L. Ritodrine- and terbutaline-induced hypokalaemia in preterm labour: Mechanisms and consequences. Kidney Int. 1997, 51, 1867–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabbat, A.; Laaban, J.P.; Boussairi, A.; Rochemaure, J. Hyperlactatemia during acute severe asthma. Intensive Care Med. 1998, 24, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Radwan, Z.M.; Ali, T.F.; Bader, H.W.; Gouda, S.M. Lactatemia during treatment of status asthmaticus in children. Egypt J. Allergy Immunol. 2004, 2, 83–89. [Google Scholar]
- Rodrigo, G.J.; Rodrigo, C. Elevated plasma lactate level associated with high dose inhaled albuterol therapy in acute severe asthma. Emerg. Med. J. 2005, 22, 404–408. [Google Scholar] [CrossRef] [Green Version]
- Meert, K.L.; McCaulley, L.; Sarnaik, A.P. Mechanism of lactic acidosis in children with acute severe asthma. Pediatr. Crit. Care Med. 2012, 13, 28–31. [Google Scholar] [CrossRef]
- Walsh, S.A.; Paget, R.I.; Ramnarayan, P. Salbutamol usage and lactic acidosis in acute severe asthma. Pediatr. Crit. Care Med. 2013, 14, 116–117. [Google Scholar] [CrossRef] [PubMed]
- Lewis, L.M.; Ferguson, I.; House, S.L.; Aubuchon, K.; Schneider, J.; Johnson, K.; Matsuda, K. Albuterol administration is commonly associated with increases in serum lactate in patients with asthma treated for acute exacerbation of asthma. Chest 2014, 145, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Appel, D.; Rubenstein, R.; Schrager, K.; Williams, M.H., Jr. Lactic acidosis in severe asthma. Am. J. Med. 1983, 75, 580–584. [Google Scholar] [CrossRef]
- Bohn, D. Metabolic acidosis in severe asthma: Is it the disease or is it the doctor? Pediatr. Crit. Care Med. 2007, 8, 582–583. [Google Scholar] [CrossRef] [PubMed]
- Qvisth, V.; Hagström-Toft, E.; Enoksson, S.; Bolinder, J. Catecholamine regulation of local lactate production in vivo in skeletal muscle and adipose tissue: Role of ß-adrenoreceptor subtypes. J. Clin. Endocrinol. Metab. 2008, 93, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatherill, M.; Salie, S.; Waggie, Z.; Lawrenson, J.; Hewitson, J.; Reynolds, L.; Argent, A. The lactate: Pyruvate ratio following open cardiac surgery in children. Intensive Care Med. 2007, 33, 822–829. [Google Scholar] [CrossRef]
- Haffner, C.A.; Kendall, M.J. Metabolic effects of ß2-agonists. J. Clin. Pharm. Ther. 1992, 17, 155–164. [Google Scholar] [CrossRef]
- Duss, G.; Bianchetti, M.G.; Cattaneo, F.A.; Mullis, P.E.; Krämer, R.; Peheim, E.; Oetliker, O.H. High proximal excretion of sodium during activation of ß2-adrenoreceptors in humans. Nephron 1993, 64, 576–579. [Google Scholar] [CrossRef]
- Barnes, P.J. Theophylline. Am. J. Respir. Crit. Care Med. 2013, 188, 901–906. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
| Gender (female:male), N | 32:15 |
| Age | |
| years | 26 [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44] |
| <18 years:≥18 years, N | 16:31 |
| Underlying Conditions | |
| Acute asthma, N | 41 |
| Intraoperative bronchospasm, N | 3 |
| Hyperkalemia, N | 1 |
| Premature labor, N | 1 |
| Voluntary intoxication, N | 1 |
| Agent | |
| Albuterol, N | 35 |
| Terbutaline, N | 2 |
| Albuterol and terbutaline, N | 7 |
| Metaproterenol, N | 1 |
| Ritodrine, N | 1 |
| Salmeterol, N | 1 |
| Route of Administration | |
| Nebulized, N | 37 |
| Intravenous, N | 3 |
| Nebulized and intravenous, N | 7 |
| Further Medication | |
| Corticosteroids, N | 41 * |
| Ipratropium, N | 25 |
| Theophylline, N | 14 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liedtke, A.G.; Lava, S.A.G.; Milani, G.P.; Agostoni, C.; Gilardi, V.; Bianchetti, M.G.; Treglia, G.; Faré, P.B. Selective ß2-Adrenoceptor Agonists and Relevant Hyperlactatemia: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 71. https://doi.org/10.3390/jcm9010071
Liedtke AG, Lava SAG, Milani GP, Agostoni C, Gilardi V, Bianchetti MG, Treglia G, Faré PB. Selective ß2-Adrenoceptor Agonists and Relevant Hyperlactatemia: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(1):71. https://doi.org/10.3390/jcm9010071
Chicago/Turabian StyleLiedtke, Alina G., Sebastiano A. G. Lava, Gregorio P. Milani, Carlo Agostoni, Viola Gilardi, Mario G. Bianchetti, Giorgio Treglia, and Pietro B. Faré. 2020. "Selective ß2-Adrenoceptor Agonists and Relevant Hyperlactatemia: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 1: 71. https://doi.org/10.3390/jcm9010071