
First-Line Administration of Fibrinogen Concentrate in the Bleeding Trauma Patient: Searching for Effective Dosages and Optimal Post-Treatment Levels Limiting Massive Transfusion—Further Results of the RETIC Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The RETIC Study Procedure
2.2. The Present Sub-Study
2.3. Statistical Analysis
3. Results
- -
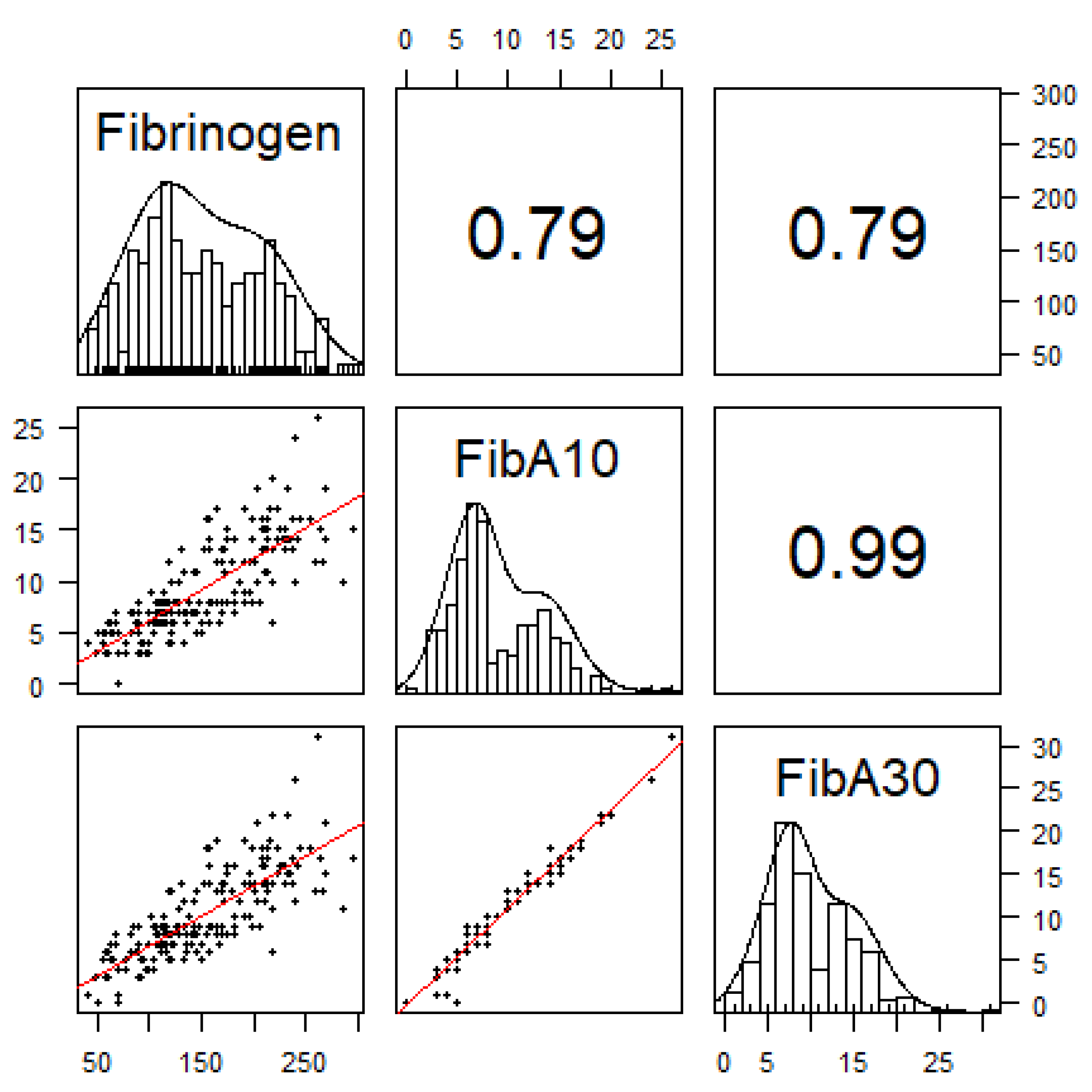
- FibA10 < 5 mm: fibrinogen concentrations < 100 mg·dL−1
- -
- FibA10 = 8 mm (study intervention threshold): fibrinogen concentrations < 150 mg·dL−1
- -
- FibA10 > 10 mm: fibrinogen concentrations > 150 mg·dL−1
- -
- FibA10 > 14 mm: fibrinogen concentrations > 200 mg·dL−1.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hiippala, S.T.; Myllyla, G.J.; Vahtera, E.M. Hemostatic Factors and Replacement of Major Blood Loss with Plasma-Poor Red Cell Concentrates. Anesth. Analg. 1995, 81, 360–365. [Google Scholar] [CrossRef]
- Tauber, H.; Innerhofer, P.; Breitkopf, R.; Westermann, I.; Beer, R.; Attal, R.E.; Strasak, A.; Mittermayr, M. Prevalence and Impact of Abnormal ROTEM® Assays in Severe Blunt Trauma: Results of the ‘Diagnosis and Treatment of Trauma-Induced Coagulopathy (DIA-TRE-TIC) Study’. Br. J. Anaesth. 2011, 107, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Rourke, C.; Curry, N.; Khan, S.; Taylor, R.; Raza, I.; Davenport, R.; Stanworth, S.; Brohi, K. Fibrinogen Levels during Trauma Hemorrhage, Response to Replacement Therapy, and Association with Patient Outcomes. J. Thromb. Haemost. 2012, 10, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Hagemo, J.S.; Stanworth, S.; Juffermans, N.P.; Brohi, K.; Cohen, M.J.; Johansson, P.I.; Røislien, J.; Eken, T.; Næss, P.A.; Gaarder, C. Prevalence, Predictors and Outcome of Hypofibrinogenaemia in Trauma: A Multicentre Observational Study. Crit. Care 2014, 18, R52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQuilten, Z.K.; Wood, E.M.; Bailey, M.; Cameron, P.A.; Cooper, D.J. Fibrinogen Is an Independent Predictor of Mortality in Major Trauma Patients: A Five-Year Statewide Cohort Study. Injury 2017, 48, 1074–1081. [Google Scholar] [CrossRef]
- Schöchl, H.; Cotton, B.; Inaba, K.; Nienaber, U.; Fischer, H.; Voelckel, W.; Solomon, C. FIBTEM Provides Early Prediction of Massive Transfusion in Trauma. Crit. Care 2011, 15, R265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Maegele, M.; Nardi, G.; Riddez, L.; et al. The European Guideline on Management of Major Bleeding and Coagulopathy Following Trauma: Fifth Edition. Crit. Care 2019, 23, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, J.; Maisch, S.; Pilshofer, L.; Streif, W.; Martini, W.; Fries, D. Fibrinogen Concentrate in Dilutional Coagulopathy: A Dose Study in Pigs. Transfusion 2014, 54, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Grottke, O.; Braunschweig, T.; Henzler, D.; Coburn, M.; Tolba, R.; Rossaint, R. Effects of Different Fibrinogen Concentrations on Blood Loss and Coagulation Parameters in a Pig Model of Coagulopathy with Blunt Liver Injury. Crit. Care 2010, 14, R62. [Google Scholar] [CrossRef] [Green Version]
- Danés, A.F.; Cuenca, L.G.; Bueno, S.R.; Barrenechea, L.M.; Ronsano, J.B.M. Efficacy and Tolerability of Human Fibrinogen Concentrate Administration to Patients with Acquired Fibrinogen Deficiency and Active or in High-risk Severe Bleeding. Vox Sang. 2008, 94, 221–226. [Google Scholar] [CrossRef]
- Fenger-Eriksen, C.; Lindberg-Larsen, M.; Christensen, A.Q.; Ingerslev, J.; Sørensen, B. Fibrinogen Concentrate Substitution Therapy in Patients with Massive Haemorrhage and Low Plasma Fibrinogen Concentrations. Br. J. Anaesth. 2008, 101, 769–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponschab, M.; Voelckel, W.; Pavelka, M.; Schlimp, C.J.; Schöchl, H. Effect of Coagulation Factor Concentrate Administration on ROTEM® Parameters in Major Trauma. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlimp, C.J.; Voelckel, W.; Inaba, K.; Maegele, M.; Schöchl, H. Impact of Fibrinogen Concentrate Alone or with Prothrombin Complex Concentrate (+/− Fresh Frozen Plasma) on Plasma Fibrinogen Level and Fibrin-Based Clot Strength (FIBTEM) in Major Trauma: A Retrospective Study. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Görlinger, K.; Fries, D.; Dirkmann, D.; Weber, C.F.; Hanke, A.A.; Schöchl, H. Reduction of Fresh Frozen Plasma Requirements by Perioperative Point-of-Care Coagulation Management with Early Calculated Goal-Directed Therapy. Transfus. Med. Hemother. 2012, 39, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Rahe-Meyer, N.; Pichlmaier, M.; Haverich, A.; Solomon, C.; Winterhalter, M.; Piepenbrock, S.; Tanaka, K.A. Bleeding Management with Fibrinogen Concentrate Targeting a High-Normal Plasma Fibrinogen Level: A Pilot Study. Br. J. Anaesth. 2009, 102, 785–792. [Google Scholar] [CrossRef] [Green Version]
- Solomon, C.; Pichlmaier, U.; Schoechl, H.; Hagl, C.; Raymondos, K.; Scheinichen, D.; Koppert, W.; Rahe-Meyer, N. Recovery of Fibrinogen after Administration of Fibrinogen Concentrate to Patients with Severe Bleeding after Cardiopulmonary Bypass Surgery. Br. J. Anaesth. 2010, 104, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Curry, N.; Foley, C.; Wong, H.; Mora, A.; Curnow, E.; Zarankaite, A.; Hodge, R.; Hopkins, V.; Deary, A.; Ray, J.; et al. Early Fibrinogen Concentrate Therapy for Major Haemorrhage in Trauma (E-FIT 1): Results from a UK Multi-Centre, Randomised, Double Blind, Placebo-Controlled Pilot Trial. Crit. Care 2018, 22, 164. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, B.; Callum, J.; Tien, H.; Peng, H.; Rizoli, S.; Karanicolas, P.; Alam, A.; Xiong, W.; Selby, R.; Garzon, A.-M.; et al. Fibrinogen in the Initial Resuscitation of Severe Trauma (FiiRST): A Randomized Feasibility Trial. Br. J. Anaesth. 2016, 117, 775–782. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, B.; Bachler, M.; Haberfellner, H.; Niederwanger, C.; Innerhofer, P.; Hell, T.; Kaufmann, M.; Maegele, M.; Martinowitz, U.; Nebl, C.; et al. Efficacy of Prehospital Administration of Fibrinogen Concentrate in Trauma Patients Bleeding or Presumed to Bleed (FIinTIC): A Multicentre, Double-Blind, Placebo-Controlled, Randomised Pilot Study. Eur. J. Anaesth. 2020, 38, 348–357. [Google Scholar] [CrossRef]
- Černý, V.; Maegele, M.; Agostini, V.; Fries, D.; Leal-Noval, S.R.; Nardai, G.; Nardi, G.; Östlund, A.; Schöchl, H. Variations and Obstacles in the Use of Coagulation Factor Concentrates for Major Trauma Bleeding across Europe: Outcomes from a European Expert Meeting. Eur. J. Trauma Emerg. Surg. 2021, 1–12. [Google Scholar] [CrossRef]
- Innerhofer, P.; Fries, D.; Mittermayr, M.; Innerhofer, N.; von Langen, D.; Hell, T.; Gruber, G.; Schmid, S.; Friesenecker, B.; Lorenz, I.H.; et al. Reversal of Trauma-Induced Coagulopathy Using First-Line Coagulation Factor Concentrates or Fresh Frozen Plasma (RETIC): A Single-Centre, Parallel-Group, Open-Label, Randomised Trial. Lancet Haematol. 2017, 4, e258–e271. [Google Scholar] [CrossRef]
- Tauber, H.; Innerhofer, N.; von Langen, D.; Ströhle, M.; Fries, D.; Mittermayr, M.; Hell, T.; Oswald, E.; Innerhofer, P. Dynamics of Platelet Counts in Major Trauma: The Impact of Haemostatic Resuscitation and Effects of Platelet Transfusion—A Sub-Study of the Randomized Controlled RETIC Trial. J. Clin. Med. 2020, 9, 2420. [Google Scholar] [CrossRef]
- Ingerslev, J.; Sørensen, B. Fibrinogen Substitution. Use in the Treatment of Bleeding Due to Lack of Fibrinogen. Ugeskr. Laeger 2005, 167, 2759–2761. [Google Scholar]
- Seebold, J.A.; Campbell, D.; Wake, E.; Walters, K.; Ho, D.; Chan, E.; Bulmer, A.C.; Wullschleger, M.; Winearls, J. Targeted Fibrinogen Concentrate Use in Severe Traumatic Haemorrhage. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2019, 21, 171–178. [Google Scholar]
- Haas, T.; Spielmann, N.; Restin, T.; Seifert, B.; Henze, G.; Obwegeser, J.; Min, K.; Jeszenszky, D.; Weiss, M.; Schmugge, M. Higher Fibrinogen Concentrations for Reduction of Transfusion Requirements during Major Paediatric Surgery: A Prospective Randomised Controlled Trial. Br. J. Anaesth. 2015, 115, 234–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolliger, D.; Szlam, F.; Molinaro, R.J.; Rahe-Meyer, N.; Levy, J.H.; Tanaka, K.A. Finding the Optimal Concentration Range for Fibrinogen Replacement after Severe Haemodilution: An in Vitro Model. Br. J. Anaesth 2009, 102, 793–799. [Google Scholar] [CrossRef] [Green Version]
- Simurda, T.; Snahnicanova, Z.; Loderer, D.; Sokol, J.; Stasko, J.; Lasabova, Z.; Kubisz, P. Fibrinogen Martin: A Novel Mutation in FGB (Gln180Stop) Causing Congenital Afibrinogenemia. Semin. Thromb. Hemost. 2016, 42, 455–458. [Google Scholar] [CrossRef] [Green Version]
- Fries, D.; Innerhofer, P.; Schobersberger, W. Time for Changing Coagulation Management in Trauma-Related Massive Bleeding. Curr. Opin. Anesthesiol. 2009, 22, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Breitkopf, R.; Westermann, I.; Tauber, H.; Mittermayr, M.; Gasteiger, L.; Dünser, M.; Innerhofer, P. FXIII Deficiency Occurs Frequently in Major Trauma and Influences Transfusion Requirements While Levels of Von Willebrand Factor Are Well above Thresholds. Emerg. Med. Investig. 2017, 2017, 51. [Google Scholar] [CrossRef]
- Innerhofer, P.; Westermann, I.; Tauber, H.; Breitkopf, R.; Fries, D.; Kastenberger, T.; Attal, R.E.; Strasak, A.; Mittermayr, M. The Exclusive Use of Coagulation Factor Concentrates Enables Reversal of Coagulopathy and Decreases Transfusion Rates in Patients with Major Blunt Trauma. Injury 2013, 44, 209–216. [Google Scholar] [CrossRef]
- Rugeri, L.; Levrat, A.; David, J.S.; Delecroix, E.; Floccard, B.; Gros, A.; Allaouchiche, B.; Negrier, C. Diagnosis of Early Coagulation Abnormalities in Trauma Patients by Rotation Thrombelastography. J. Thromb. Haemost. 2007, 5, 289–295. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.J.; Veen, C.S.B.; Snoek, C.J.M.; Kruip, M.J.H.A.; de Maat, M.P.M. FIBTEM Clot Firmness Parameters Correlate Well with the Fibrinogen Concentration Measured by the Clauss Assay in Patients and Healthy Subjects. Scand. J. Clin. Lab. Investig. 2020, 80, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.T.; Nascimento, B.; Tien, H.; Callum, J.; Rizoli, S.; Rhind, S.G.; Beckett, A. A Comparative Study of Viscoelastic Hemostatic Assays and Conventional Coagulation Tests in Trauma Patients Receiving Fibrinogen Concentrate. Clin. Chim. Acta 2019, 495, 253–262. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 70) | |
|---|---|
| Age (ys) | 43 (26 to 53) |
| Male sex (n) | 49/70 (70%) |
| BMI (kg⋅m−2) | 24.7 (22.9 to 26.2) |
| Time to ED (min) | 60 (41 to 87) |
| ISS (pts) | 35 (29–45) |
| Brain injury (n) | 33/70 (47.1%) |
| AIS brain > 2 (n) | 23/70 (32.9%) |
| GCS (pts) | 12 (9–15) |
| Prehospital TXA (n) | 6/70 (8.6%) |
| Intubation (n) | 39/70 (55.7%) |
| Systolic BP (mm Hg) | 101 (79 to 130) |
| Systolic BP < 90 mm Hg (n) | 25/70 (35.7%) |
| Heart rate (bts⋅min−1) | 105 (82 to 116) |
| pH | 7.32 (7.24 to 7.36) |
| PH < 7.35 (n) | 46/70 (65.7%) |
| BD (mmol·L−1) | 4.45 (2.92 to 7.18) |
| BD < 6 (n) | 50/70 (71.4%) |
| Hb (g·L−1) | 112 (95 to 13) |
| PTI (%) | 65.5 (51 to 76.5) |
| INR | 1.3 (1.2 to 1.5) |
| aPTT (s) | 33 (29 to 39.8) |
| Fibrinogen (mg·dL−1) | 189 (128 to 219) |
| Platelets (G⋅L−1) | 182 (153 to 213) |
| ExCT (s) | 58 (51 to 69) |
| ExA10 (mm) | 46 (39 to 50) |
| FibA10 (mm) | 8 (5 to 10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Innerhofer, N.; Treichl, B.; Rugg, C.; Fries, D.; Mittermayr, M.; Hell, T.; Oswald, E.; Innerhofer, P.; on behalf of the RETIC Study Group. First-Line Administration of Fibrinogen Concentrate in the Bleeding Trauma Patient: Searching for Effective Dosages and Optimal Post-Treatment Levels Limiting Massive Transfusion—Further Results of the RETIC Study. J. Clin. Med. 2021, 10, 3930. https://doi.org/10.3390/jcm10173930
Innerhofer N, Treichl B, Rugg C, Fries D, Mittermayr M, Hell T, Oswald E, Innerhofer P, on behalf of the RETIC Study Group. First-Line Administration of Fibrinogen Concentrate in the Bleeding Trauma Patient: Searching for Effective Dosages and Optimal Post-Treatment Levels Limiting Massive Transfusion—Further Results of the RETIC Study. Journal of Clinical Medicine. 2021; 10(17):3930. https://doi.org/10.3390/jcm10173930
Chicago/Turabian StyleInnerhofer, Nicole, Benjamin Treichl, Christopher Rugg, Dietmar Fries, Markus Mittermayr, Tobias Hell, Elgar Oswald, Petra Innerhofer, and on behalf of the RETIC Study Group. 2021. "First-Line Administration of Fibrinogen Concentrate in the Bleeding Trauma Patient: Searching for Effective Dosages and Optimal Post-Treatment Levels Limiting Massive Transfusion—Further Results of the RETIC Study" Journal of Clinical Medicine 10, no. 17: 3930. https://doi.org/10.3390/jcm10173930