
Psychometric Properties of the Proxy-Reported Life-Space Assessment in Institutionalized Settings (LSA-IS-Proxy) for Older Persons with and without Cognitive Impairment

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Descriptive Measures
2.2. Life-Space Mobility Assessment
2.3. Assessment of Measurement Properties and Assessment Procedure
2.4. Subgroup Analyses
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
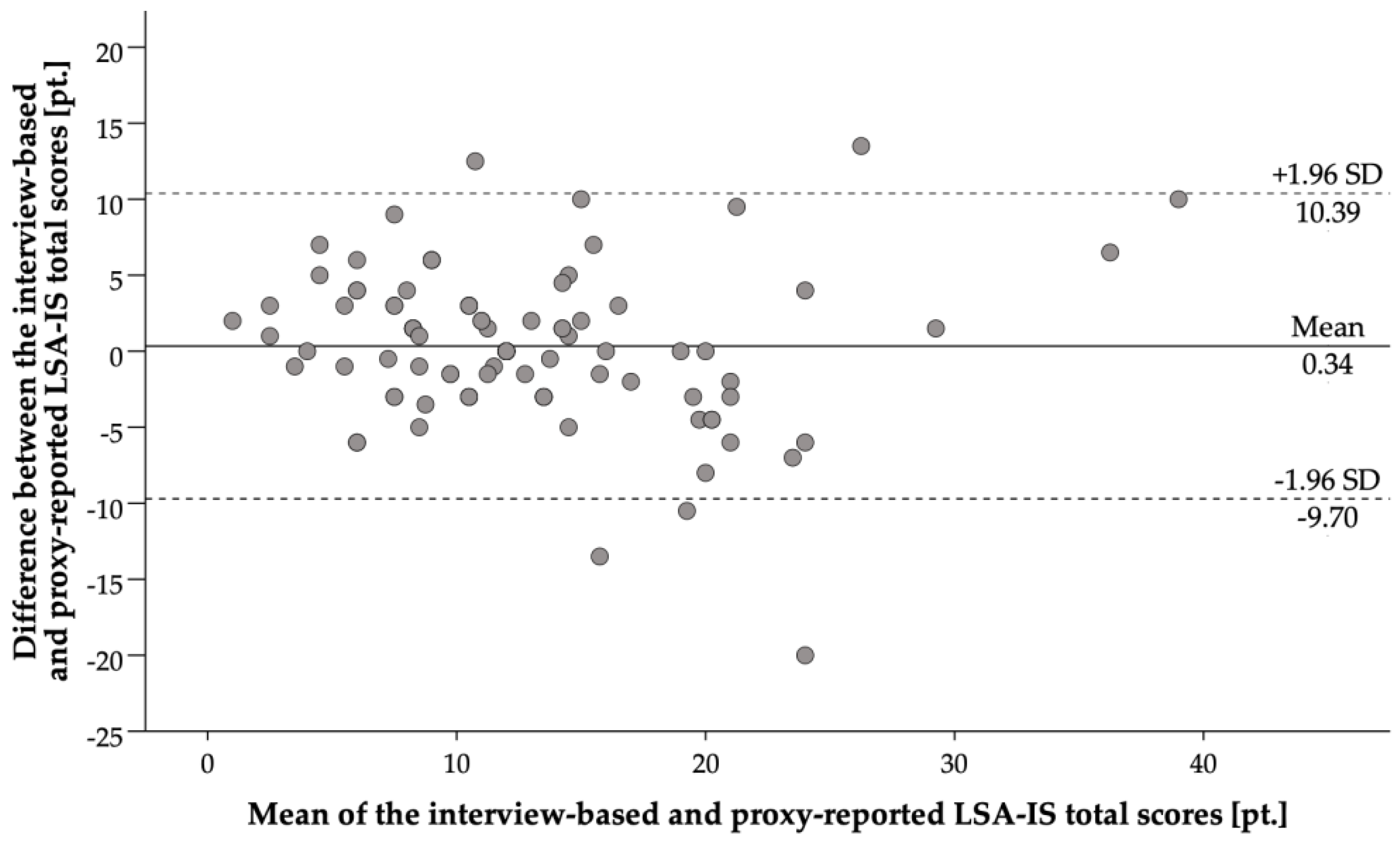
3.2. Concurrent Validity
3.3. Construct Validity
3.4. Test-Retest Reliability
3.5. Sensitivity to Change
3.6. Feasibility
4. Discussion
4.1. Concurrent Validity
4.2. Construct Validity
4.3. Test-Retest Reliability
4.4. Sensitivity to Change
4.5. Feasibility
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Webber, S.C.; Porter, M.M.; Menec, V.H. Mobility in older adults: A comprehensive framework. Gerontologyist 2010, 50, 443–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, M.; Baker, P.S.; Allman, R.M. A Life-Space Approach to Functional Assessment of Mobility in the Elderly. J. Gerontol. Soc. Work 2002, 35, 35–55. [Google Scholar] [CrossRef]
- Satariano, W.A.; Guralnik, J.M.; Jackson, R.J.; Marottoli, R.A.; Phelan, E.A.; Prohaska, T.R. Mobility and aging: New directions for public health action. Am. J. Public Health 2012, 102, 1508–1515. [Google Scholar] [CrossRef] [PubMed]
- Metz, D.H. Mobility of older people and their quality of life. Transp. Policy 2000, 7, 149–152. [Google Scholar] [CrossRef]
- Barnes, L.L.; Wilson, R.S.; Bienias, J.L.; de Leon, C.F.; Kim, H.J.; Buchman, A.S.; Bennett, D.A. Correlates of life space in a volunteer cohort of older adults. Exp. Aging Res. 2007, 33, 77–93. [Google Scholar] [CrossRef]
- Rosso, A.L.; Taylor, J.A.; Tabb, L.P.; Michael, Y.L. Mobility, disability, and social engagement in older adults. J. Aging Health 2013, 25, 617–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.J.; Redden, D.T.; Flood, K.L.; Allman, R.M. The underrecognized epidemic of low mobility during hospitalization of older adults. J. Am. Geriatr. Soc. 2009, 57, 1660–1665. [Google Scholar] [CrossRef]
- den Ouden, M.; Bleijlevens, M.H.C.; Meijers, J.M.M.; Zwakhalen, S.M.G.; Braun, S.M.; Tan, F.E.S.; Hamers, J.P.H. Daily (In)Activities of Nursing Home Residents in Their Wards: An Observation Study. J. Am. Med. Dir. Assoc. 2015, 16, 963–968. [Google Scholar] [CrossRef]
- Brown, C.J.; Friedkin, R.J.; Inouye, S.K. Prevalence and outcomes of low mobility in hospitalized older patients. J. Am. Geriatr. Soc. 2004, 52, 1263–1270. [Google Scholar] [CrossRef]
- May, D.; Nayak, U.S.; Isaacs, B. The life-space diary: A measure of mobility in old people at home. Int. Rehabil. Med. 1985, 7, 182–186. [Google Scholar] [CrossRef]
- Johnson, J.; Rodriguez, M.A. Life-Space Mobility in the Elderly: Current Perspectives. Clin. Interv. Aging 2020, 15, 1665–1674. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.K.; Buchan, I.E.; van der Veer, S.N. Assessing life-space mobility for a more holistic view on wellbeing in geriatric research and clinical practice. Aging Clin. Exp. Res. 2019, 31, 439–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.J.; Williams, B.R.; Woodby, L.L.; Davis, L.L.; Allman, R.M. Barriers to mobility during hospitalization from the perspectives of older patients and their nurses and physicians. J. Hosp. Med. 2007, 2, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Jansen, C.P.; Diegelmann, M.; Schnabel, E.L.; Wahl, H.W.; Hauer, K. Life-space and movement behavior in nursing home residents: Results of a new sensor-based assessment and associated factors. BMC Geriatr. 2017, 17, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, T.M.; Allore, H.G.; Holford, T.R.; Guo, Z. Hospitalization, restricted activity, and the development of disability among older persons. JAMA 2004, 292, 2115–2124. [Google Scholar] [CrossRef] [Green Version]
- Luppa, M.; Luck, T.; Weyerer, S.; Konig, H.H.; Brahler, E.; Riedel-Heller, S.G. Prediction of institutionalization in the elderly. A systematic review. Age Ageing 2010, 39, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Bickel, H.; Hendlmeier, I.; Heßler, J.B.; Junge, M.N.; Leonhardt-Achilles, S.; Weber, J.; Schäufele, M. The Prevalence of Dementia and Cognitive Impairment in Hospitals. Dtsch. Arztebl. Int. 2018, 115, 733–740. [Google Scholar] [CrossRef]
- Kim, S.; Miller, M.E.; Lin, M.; Rejeski, W.J.; Kritchevsky, S.B.; Marsh, A.P.; Groban, L. Self- vs proxy-reported mobility using the mobility assessment tool-short form in elderly preoperative patients. Eur. Rev. Aging Phys. Act. Off. J. Eur. Group Res. Elder. Phys. Act. 2018, 15, 5. [Google Scholar] [CrossRef] [Green Version]
- Lukas, A.; Niederecker, T.; Günther, I.; Mayer, B.; Nikolaus, T. Self- and proxy report for the assessment of pain in patients with and without cognitive impairment Experiences gained in a geriatric hospital. Z. Gerontol. Geriatr. 2013, 46. [Google Scholar] [CrossRef]
- Gerritsen, D.L.; Steverink, N.; Ooms, M.E.; de Vet, H.C.W.; Ribbe, M.W. Measurement of overall quality of life in nursing homes through self-report: The role of cognitive impairment. Qual. Life Res. 2007, 16, 1029–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauer, K.; Ullrich, P.; Heldmann, P.; Hummel, S.; Bauer, J.M.; Werner, C. Validation of the interview-based life-space assessment in institutionalized settings (LSA-IS) for older persons with and without cognitive impairment. BMC Geriatr. 2020, 20, 534. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Ginter, S.F. The nursing home life-space diameter. A measure of extent and frequency of mobility among nursing home residents. J. Am. Geriatr. Soc. 1990, 38, 1311–1315. [Google Scholar] [CrossRef] [PubMed]
- Dutzi, I.; Schwenk, M.; Kirchner, M.; Bauer, J.M.; Hauer, K. “What would you like to achieve?” Goal-Setting in Patients with Dementia in Geriatric Rehabilitation. BMC Geriatr 2019, 19, 280. [Google Scholar] [CrossRef] [Green Version]
- Macháčová, K.; Vaňková, H.; Holmerová, I.; Čábelková, I.; Volicer, L. Ratings of activities of daily living in nursing home residents: Comparison of self- and proxy ratings with actual performance and the impact of cognitive status. Eur. J. Ageing 2018, 15, 349–358. [Google Scholar] [CrossRef]
- Hauer, K.; Yardley, L.; Beyer, N.; Kempen, G.; Dias, N.; Campbell, M.; Becker, C.; Todd, C. Validation of the Falls Efficacy Scale and Falls Efficacy Scale International in geriatric patients with and without cognitive impairment: Results of self-report and interview-based questionnaires. Gerontology 2010, 56, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Iezzoni, L.I.; McCarthy, E.P.; Davis, R.B.; Siebens, H. Mobility problems and perceptions of disability by self-respondents and proxy respondents. Med. Care 2000, 38, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Lapin, B.R.; Thompson, N.R.; Schuster, A.; Katzan, I.L. Patient versus proxy response on global health scales: No meaningful DIFference. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2019, 28, 1585–1594. [Google Scholar] [CrossRef]
- Pfisterer, M.H.; Johnson, T.M., 2nd; Jenetzky, E.; Hauer, K.; Oster, P. Geriatric patients’ preferences for treatment of urinary incontinence: A study of hospitalized, cognitively competent adults aged 80 and older. J. Am. Geriatr. Soc. 2007, 55, 2016–2022. [Google Scholar] [CrossRef]
- Howland, M.; Allan, K.C.; Carlton, C.E.; Tatsuoka, C.; Smyth, K.A.; Sajatovic, M. Patient-rated versus proxy-rated cognitive and functional measures in older adults. Patient Relat. Outcome Meas. 2017, 8, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, N.; Zimmerman, S.; Hawkes, W.G.; Gruber-Baldini, A.L.; Hebel, J.R.; Magaziner, J. Concordance of proxy-perceived change and measured change in multiple domains of function in older persons. J. Am. Geriatr. Soc. 2004, 52, 1157–1162. [Google Scholar] [CrossRef]
- Magaziner, J.; Zimmerman, S.I.; Gruber-Baldini, A.L.; Hebel, J.R.; Fox, K.M. Proxy reporting in five areas of functional status. Comparison with self-reports and observations of performance. Am. J. Epidemiol. 1997, 146, 418–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Harris, I.; Lu, Z.K. Differences in proxy-reported and patient-reported outcomes: Assessing health and functional status among medicare beneficiaries. BMC Med. Res. Methodol. 2015, 15, 62. [Google Scholar] [CrossRef] [Green Version]
- Cavanaugh, J.T.; Crawford, K. Life-Space Assessment and Physical Activity Scale for the Elderly: Validity of proxy informant responses. Arch. Phys. Med. Rehabil. 2014, 95, 1527–1532. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.S.; Bodner, E.V.; Allman, R.M. Measuring life-space mobility in community-dwelling older adults. J. Am. Geriatr. Soc. 2003, 51, 1610–1614. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Inouye, S.K.; van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauer, K.; Lamb, S.; Jorstad, E.; Todd, C.; Becker, C.; PROFANE-Group. Systematic review of definitions and methods of measuring falls in randomised controlled fall prevention trials. Age Ageing 2006, 35, 5–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrell, B.A.; Ferrell, B.R.; Rivera, L. Pain in cognitively impaired nursing home patients. J. Pain Symptom Manag. 1995, 10, 591–598. [Google Scholar] [CrossRef]
- Schuler, M.; Njoo, N.; Hestermann, M.; Oster, P.; Hauer, K. Acute and chronic pain in geriatrics: Clinical characteristics of pain and the influence of cognition. Pain Med. 2004, 5, 253–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogullari, S. Reliability and validity of the Apathy Evaluation Scale. Psychiatry Res. 1991, 38, 143–162. [Google Scholar] [CrossRef]
- Lueken, U.; Seidl, U.; Völker, L.; Schweiger, E.; Kruse, A.; Schröder, J. Development of a short version of the Apathy Evaluation Scale specifically adapted for demented nursing home residents. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2007, 15, 376–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauer, K.; Kempen, G.I.; Schwenk, M.; Yardley, L.; Beyer, N.; Todd, C.; Oster, P.; Zijlstra, G.A. Validity and sensitivity to change of the falls efficacy scales international to assess fear of falling in older adults with and without cognitive impairment. Gerontology 2011, 57, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Kempen, G.I.; Yardley, L.; van Haastregt, J.C.; Zijlstra, G.A.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: the barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Bongartz, M.; Kiss, R.; Lacroix, A.; Eckert, T.; Ullrich, P.; Jansen, C.P.; Feisst, M.; Mellone, S.; Chiari, L.; Becker, C.; et al. Validity, reliability, and feasibility of the uSense activity monitor to register physical activity and gait performance in habitual settings of geriatric patients. Physiol. Meas. 2019, 40, 095005. [Google Scholar] [CrossRef]
- Ullrich, P.; Werner, C.; Bongartz, M.; Kiss, R.; Bauer, J.; Hauer, K. Validation of a Modified Life-Space Assessment in Multimorbid Older Persons With Cognitive Impairment. Gerontologist 2019, 59, e66–e75. [Google Scholar] [CrossRef]
- McHorney, C.A.; Tarlov, A.R. Individual-patient monitoring in clinical practice: Are available health status surveys adequate? Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 1995, 4, 293–307. [Google Scholar] [CrossRef]
- Fleiss, J.L. The Design and Analysis of Clinical Experiments; John Wiley & Sons: New York, NY, USA, 1986. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Laurence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar] [CrossRef]
- Katz, J.N.; Larson, M.G.; Phillips, C.B.; Fossel, A.H.; Liang, M.H. Comparative measurement sensitivity of short and longer health status instruments. Med. Care 1992, 30, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Middel, B.; van Sonderen, E. Statistical significant change versus relevant or important change in (quasi) experimental design: Some conceptual and methodological problems in estimating magnitude of intervention-related change in health services research. Int. J. Integr. Care 2002, 2, e15. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Yamagami, T. Life-space and Related Factors for the Elderly in a Geriatric Health Service Facility. Prog. Rehabil. Med. 2018, 3, 20180001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakshaug, J.W. Proxy Reporting in Health Surveys. In T.P. Johnson, Health Survey Methods; John Wiley & Sons: New York, NY, USA, 2014; pp. 367–381. [Google Scholar] [CrossRef]
- Peel, C.; Baker, P.S.; Roth, D.L.; Brown, C.J.; Bodner, E.V.; Allman, R.M. Assessing mobility in older adults: The UAB Study of Aging Life-Space Assessment. Phys. Ther. 2005, 85, 1008–1019. [Google Scholar] [CrossRef] [Green Version]
- Umstattd Meyer, M.R.; Janke, M.C.; Beaujean, A.A. Predictors of older adults’ personal and community mobility: Using a comprehensive theoretical mobility framework. Gerontologist 2014, 54, 398–408. [Google Scholar] [CrossRef] [Green Version]
- Kuspinar, A.; Verschoor, C.P.; Beauchamp, M.K.; Dushoff, J.; Ma, J.; Amster, E.; Bassim, C.; Dal Bello-Haas, V.; Gregory, M.A.; Harris, J.E.; et al. Modifiable factors related to life-space mobility in community-dwelling older adults: Results from the Canadian Longitudinal Study on Aging. BMC Geriatr. 2020, 20, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullrich, P.; Eckert, T.; Bongartz, M.; Werner, C.; Kiss, R.; Bauer, J.M.; Hauer, K. Life-space mobility in older persons with cognitive impairment after discharge from geriatric rehabilitation. Arch. Gerontol. Geriatr. 2018, 81, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Seinsche, J.; Zijlstra, W.; Giannouli, E. Motility in Frail Older Adults: Operationalization of a New Framework and First Insights into Its Relationship with Physical Activity and Life-Space Mobility: An Exploratory Study. Int. J. Environ. Res. Public Health 2020, 17, 8814. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F.; Kaduszkiewicz, H.; Glaeske, G.; van den Bussche, H.; Koller, D. Prevalence of dementia in nursing home and community-dwelling older adults in Germany. Aging Clin. Exp. Res. 2014, 26, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Busse, M.E.; Tyson, S.F. Functional balance and mobility tests in healthy participants: Reliability, error and influencing factors. Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2007, 12, 242–250. [Google Scholar] [CrossRef]
- Trautwein, S.; Maurus, P.; Barisch-Fritz, B.; Hadzic, A.; Woll, A. Recommended motor assessments based on psychometric properties in individuals with dementia: A systematic review. Eur. Rev. Aging Phys. Act. Off. J. Eur. Group Res. Elder. Phys. Act. 2019, 16, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gell, N.M.; Wallace, R.B.; LaCroix, A.Z.; Mroz, T.M.; Patel, K.V. Mobility Device Use in Older Adults and Incidence of Falls and Worry About Falling: Findings from the 2011–2012 National Health and Aging Trends Study. J. Am. Geriatr. Soc. 2015, 63, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Quisenberry, A.J.; Snider, S.E.; Bickel, W.K. The Return of Rate Dependence. Behav. Anal. 2016, 16, 215–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laughlin, M.H.; Joseph, B. Wolfe Memorial lecture. Physical activity in prevention and treatment of coronary disease: The battle line is in exercise vascular cell biology. Med. Sci. Sports Exerc. 2004, 36, 352–362. [Google Scholar] [CrossRef]
- Werner, C.; Rosner, R.; Wiloth, S.; Lemke, N.C.; Bauer, J.M.; Hauer, K. Time course of changes in motor-cognitive exergame performances during task-specific training in patients with dementia: Identification and predictors of early training response. J. Neuroeng. Rehabil. 2018, 15, 100. [Google Scholar] [CrossRef] [Green Version]
- Ullrich, P.; Werner, C.; Bongartz, M.; Eckert, T.; Abel, B.; Schönstein, A.; Kiss, R.; Hauer, K. Increasing Life-Space Mobility in community-dwelling older persons with cognitive impairment following rehabilitation: A randomized controlled trial. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total Sample (n = 94) | Persons without CI (n = 48) | Persons with CI (n = 46) |
|---|---|---|---|
| Gender (female) | 58 (61.7) | 31 (64.6) | 27 (58.7) |
| Age (years) | 83.3 (6.1) | 82.3 (5.9) | 84.4 (6.2) |
| Number of medications | 9.9 (4.0) | 9.5 (4.0) | 10.2 (4.0) |
| CFS | 5.5 (1.0) | 5.2 (0.9) | 5.8 (1.0) |
| PPI | 1.4 (1.5) | 1.2 (1.3) | 1.6 (1.7) |
| MMSE | 22.8 (4.8) | 26.7 (1.7) | 18.8 (3.4) |
| EQ-5D | 0.65 (0.31) | 0.69 (0.28) | 0.58 (0.33) |
| AES-C | 24.3 (8.6) | 26.7 (7.9) | 21.7 (8.7) |
| Short-FES-I | 12 [7–28] | 11 [7–25] | 12 [7–28] |
| Falls in the previous year | 1.2 (0.8) | 1.1 (0.8) | 1.2 (0.8) |
| ADL Barthel-Index | 75 [5–100] | 85 [25–100] | 65 [5–100] |
| SPPB | 4.2 (2.4) | 4.6 (2.3) | 3.8 (2.5) |
| Number of steps in 48 h (uSense) | 2560 (3361) | 3115 (3642) | 1960 (2961) |
| LSA-IS-proxy scores | |||
| Total score | 12.7 (7.1) | 14.4 (8.3) | 11.0 (5.2) |
| Maximal life-space | 2.2 (0.7) | 2.3 (0.7) | 2.1 (0.8) |
| Equipment-assisted life-space | 1.7 (1.0) | 2.0 (0.9) | 1.4 (1.0) |
| Independent life-space | 0.4 (0.8) | 0.4 (0.8) | 0.4 (0.7) |
| Self-Reported LSA-IS Scores | LSA-IS-Proxy Scores | |||
|---|---|---|---|---|
| Total Score | Maximal Life-Space | Equipment-Assisted Life-Space | Independent Life-Space | |
| Total score | ||||
| total group | 0.77 (0.67–0.84) | |||
| without CI | 0.79 (0.66–0.88) | |||
| with CI | 0.69 (0.50–0.82) | |||
| Maximal life-space | ||||
| total group | 0.65 (0.51–0.57) | |||
| without CI | 0.56 (0.33–0.73) | |||
| with CI | 0.71 (0.52–0.83) | |||
| Equipment-assisted life-space | ||||
| total group | 0.59 (0.44–0.71) | |||
| without CI | 0.54 (0.31–0.72) | |||
| with CI | 0.55 (0.32–0.73) | |||
| Independent life-space | ||||
| total group | 0.70 (0.58–0.79) | |||
| without CI | 0.79 (0.66–0.88) | |||
| with CI | 0.61 (0.39–0.76) | |||
| LSA-IS-Proxy Scores | |||||
|---|---|---|---|---|---|
| Variables | Group | Total Score | Maximal Life-Space | Equipment-Assisted Life-Space | Independent Life-Space |
| Demographic factors | |||||
| Age | total group | −0.31 * | −0.10 | −0.37 * | −0.20 |
| without CI | −0.32 * | −0.06 | −0.21 | −0.24 | |
| with CI | −0.26 | −0.10 | −0.43 ** | −0.16 | |
| Gender 1 | total group | −0.05 | 0.02 | 0.05 | −0.05 |
| without CI | −0.06 | 0.05 | 0.12 | −0.20 | |
| with CI | −0.01 | 0.01 | −0.04 | 0.01 | |
| Health status | |||||
| No. of medication | total group | −0.13 | −0.04 | −0.02 | −0.13 |
| without CI | −0.13 | −0.04 | 0.08 | 0.08 | |
| with CI | 0.10 | −0.01 | −0.06 | −0.15 | |
| CFS | total group | −0.41 ** | −0.21 | −0.56 ** | −0.46 ** |
| without CI | −0.30 * | −0.22 | −0.43 ** | −0.32 * | |
| with CI | −0.44 ** | −0.21 | −0.60 ** | −0.60 ** | |
| PPI | total group | −0.10 | 0.02 | −0.27 * | 0.12 |
| without CI | −0.04 | −0.16 | −0.21 | 0.21 | |
| with CI | −0.12 | 0.11 | −0.27 | 0.04 | |
| Cognitive Status | |||||
| MMSE | total group | 0.21 * | 0.13 | 0.30 ** | −0.02 |
| without CI | 0.22 | 0.13 | 0.13 | −0.01 | |
| with CI | −0.13 | −0.14 | 0.09 | −0.09 | |
| Psychosocial status | |||||
| EQ-5D | total group | 0.30 ** | 0.22* | 0.43 ** | 0.21 |
| without CI | 0.16 | 0.30* | 0.45 ** | 0.07 | |
| with CI | 0.34 * | 0.10 | 0.39 ** | 0.29 | |
| AES-C | total group | 0.23 * | 0.14 | 0.36 ** | 0.13 |
| without CI | 0.27 | 0.09 | 0.43 ** | 0.08 | |
| with CI | 0.07 | 0.13 | 0.14 | 0.21 | |
| Short-FES-I | total group | −0.18 | −0.15 | −0.37 ** | −0.13 |
| without CI | −0.08 | −0.21 | −0.48 ** | −0.03 | |
| with CI | −0.25 | −0.08 | −0.31 * | −0.25 | |
| Motor-functional status | |||||
| ADL Barthel Index | total group | 0.47 ** | 0.20 | 0.66 ** | 0.35 ** |
| without CI | 0.40 ** | 0.25 | 0.61 ** | 0.26 | |
| with CI | 0.46 ** | 0.14 | 0.65 ** | 0.47 ** | |
| SPPB | total group | 0.50 ** | 0.25 * | 0.59 ** | 0.43 ** |
| without CI | 0.39 ** | 0.21 | 0.51 ** | 0.32 * | |
| with CI | 0.56 ** | 0.28 | 0.60 ** | 0.57 ** | |
| Physical activity | |||||
| Duration of activity | total group | 0.41 ** | 0.13 | 0.55 ** | 0.29 ** |
| without CI | 0.34 * | 0.16 | 0.47 ** | 0.24 | |
| with CI | 0.38 * | −0.01 | 0.53 ** | 0.36 * | |
| Duration of gait | total group | 0.53 * | 0.19 | 0.56 ** | 0.43 ** |
| without CI | 0.46 ** | 0.24 | 0.52 ** | 0.48 ** | |
| with CI | 0.58 ** | 0.10 | 0.60 ** | 0.40 ** | |
| No. of steps | total group | 0.30 ** | 0.20 | 0.55 ** | 0.41 ** |
| without CI | 0.45 ** | 0.26 | 0.53 ** | 0.44 ** | |
| with CI | 0.59 ** | 0.10 | 0.54 ** | 0.40 ** | |
| LSA-IS-Proxy Scores | Group | Mean (SD) | ICC (95% Confidence Interval) | |
|---|---|---|---|---|
| Test | Retest | |||
| Total score | total group | 14.45 (8.58) | 14.50 (8.74) | 0.74 (0.63–0.82) |
| without CI | 16.32 (10.17) | 15.53 (7.95) | 0.68 (0.45–0.82) | |
| with CI | 13.01 (6.90) | 13.71 (9.31) | 0.80 (0.67–0.88) | |
| Maximal life-space | total group | 2.31 (0.74) | 2.34 (0.81) | 0.44 (0.25–0.60) |
| without CI | 2.43 (0.73) | 2.38 (0.64) | 0.36 (0.04–0.61) | |
| with CI | 2.21 (0.74) | 2.31 (0.93) | 0.48 (0.23–0.67) | |
| Equipment-assisted life-space | total group | 1.92 (1.04) | 1.82 (1.16) | 0.76 (0.65–0.83) |
| without CI | 2.24 (0.93) | 2.03 (0.96) | 0.52 (0.24–0.72) | |
| with CI | 1.67 (1.06) | 1.67 (1.28) | 0.86 (0.77–0.92) | |
| Independent life-space | total group | 0.48 (0.95) | 0.47 (0.91) | 0.87 (0.81–0.91) |
| without CI | 0.57 (1.04) | 0.51 (0.90) | 0.83 (0.69–0.91) | |
| with CI | 0.42 (0.87) | 0.44 (0.92) | 0.91 (0.84–0.95) | |
| LSA-IS-Proxy Scores | Group | Mean (SD) | p-Value | SRM | |
|---|---|---|---|---|---|
| Baseline | Post-Intervention | ||||
| Total score | total group | 13.80 (7.87) | 17.70 (9.40) | >0.001 | 0.44 |
| without CI | 15.13 (8.90) | 18.52 (8.34) | 0.048 | 0.39 | |
| with CI | 12.78 (6.92) | 17.08 (10.21) | >0.001 | 0.45 | |
| Maximal life-space | total group | 2.17 (0.73) | 2.54 (0.80) | 0.001 | 0.47 |
| without CI | 2.27 (0.74) | 2.50 (0.73) | 0.109 | 0.32 | |
| with CI | 2.10 (0.72) | 2.56 (0.85) | 0.006 | 0.58 | |
| Equipment-assisted life-space | total group | 1.83 (0.94) | 2.23 (1.09) | >0.001 | 0.40 |
| without CI | 1.93 (0.98) | 2.37 (0.96) | 0.021 | 0.45 | |
| with CI | 1.74 (0.91) | 2.13 (1.17) | 0.002 | 0.35 | |
| Independent life-space | total group | 0.46 (0.88) | 0.59 (1.06) | 0.151 | 0.13 |
| without CI | 0.50 (0.97) | 0.57 (0.97) | 0.601 | 0.07 | |
| with CI | 0.44 (0.82) | 0.62 (1.14) | 0.164 | 0.17 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hauer, K.; Ullrich, P.; Heldmann, P.; Bauknecht, L.; Hummel, S.; Abel, B.; Bauer, J.M.; Lamb, S.E.; Werner, C. Psychometric Properties of the Proxy-Reported Life-Space Assessment in Institutionalized Settings (LSA-IS-Proxy) for Older Persons with and without Cognitive Impairment. Int. J. Environ. Res. Public Health 2021, 18, 3872. https://doi.org/10.3390/ijerph18083872
Hauer K, Ullrich P, Heldmann P, Bauknecht L, Hummel S, Abel B, Bauer JM, Lamb SE, Werner C. Psychometric Properties of the Proxy-Reported Life-Space Assessment in Institutionalized Settings (LSA-IS-Proxy) for Older Persons with and without Cognitive Impairment. International Journal of Environmental Research and Public Health. 2021; 18(8):3872. https://doi.org/10.3390/ijerph18083872
Chicago/Turabian StyleHauer, Klaus, Phoebe Ullrich, Patrick Heldmann, Laura Bauknecht, Saskia Hummel, Bastian Abel, Juergen M. Bauer, Sarah E. Lamb, and Christian Werner. 2021. "Psychometric Properties of the Proxy-Reported Life-Space Assessment in Institutionalized Settings (LSA-IS-Proxy) for Older Persons with and without Cognitive Impairment" International Journal of Environmental Research and Public Health 18, no. 8: 3872. https://doi.org/10.3390/ijerph18083872