How Physical Activity across the Lifespan Can Reduce the Impact of Bone Ageing: A Literature Review

 and
and 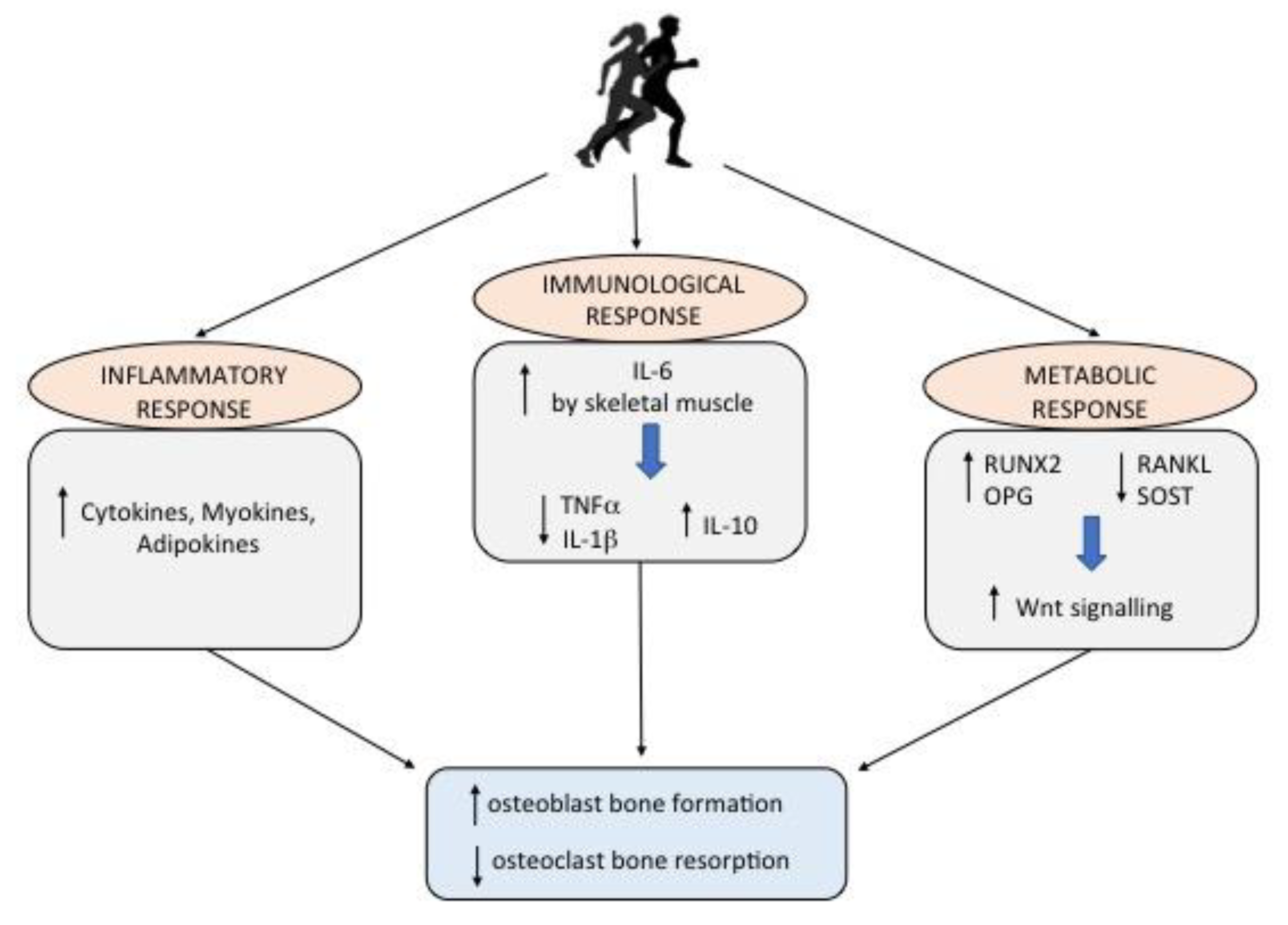{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Physiological Mechanisms of Bone Remodeling
3. Physical Activity and Bone Health: The Metabolic, Inflammatory and Immune Response
4. Impact of Physical Activity in Reducing Bone Ageing
Physical Activity during the Lifespan
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Owen, R.; Reilly, G.C. In vitro Models of Bone Remodelling and Associated Disorders. Front. Bioeng. Biotechnol. 2018, 6, 134. [Google Scholar] [CrossRef]
- Parra-Torres, A.Y.; Valdés-Flores, M.; Orozco, L.; Velázquez-Cruz, R. Molecular Aspects of Bone Remodeling. Top. Osteoporos. 2013, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Raggatt, L.J.; Partridge, N.C. Cellular and Molecular Mechanisms of Bone Remodeling. J. Biol. Chem. 2010, 285, 25103–25108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crockett, J.C.; Rogers, M.J.; Coxon, F.P.; Hocking, L.J.; Helfrich, M.H. Bone remodelling at a glance. J. Cell Sci. 2011, 124, 991–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuo, C.; Huang, Y.; Bajis, R.; Sahih, M.; Li, Y.P.; Dai, K.; Zhang, X. Osteoblastogenesis regulation signals in bone remodeling. Osteoporos. Int. 2012, 23, 1653–1663. [Google Scholar] [CrossRef] [PubMed]
- Theill, L.E.; Boyle, W.J.; Penninger, J.M. RANK-L and RANK: T cells, bone loss, and mammalian evolution. Annu. Rev. Immunol. 2002, 20, 795–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunetti, G.; D’Amato, G.; Chiarito, M.; Tullo, A.; Colaianni, G.; Colucci, S.; Grano, M.; Faienza, M.F. An update on the role of RANKL-RANK/osteoprotegerin and WNT-ß-catenin signaling pathways in pediatric diseases. World J. Pediatr. 2019, 15, 4–11. [Google Scholar] [CrossRef]
- Brunetti, G.; Grugni, G.; Piacente, L.; Delvecchio, M.; Ventura, A.; Giordano, P.; Grano, M.; D’Amato, G.; Laforgia, D.; Crinò, A.; et al. Analysis of Circulating Mediators of Bone Remodeling in Prader-Willi Syndrome. Calcif. Tissue Int. 2018, 102, 635–643. [Google Scholar] [CrossRef]
- Brunetti, G.; Tummolo, A.; D’Amato, G.; Gaeta, A.; Ortolani, F.; Piacente, L.; Giordano, P.; Colucci, S.; Grano, M.; Papadia, F.; et al. Mechanisms of Enhanced Osteoclastogenesis in Alkaptonuria. Am. J. Pathol. 2018, 188, 1059–1068. [Google Scholar] [CrossRef] [Green Version]
- Faienza, M.F.; Ventura, A.; Delvecchio, M.; Fusillo, A.; Piacente, L.; Aceto, G.; Colaianni, G.; Colucci, S.; Cavallo, L.; Grano, M.; et al. High Sclerostin and Dickkopf-1 (DKK-1) Serum Levels in Children and Adolescents with Type 1 Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2017, 102, 1174–1181. [Google Scholar] [CrossRef] [Green Version]
- Brunetti, G.; Papadia, F.; Tummolo, A.; Fischetto, R.; Nicastro, F.; Piacente, L.; Ventura, A.; Mori, G.; Oranger, A.; Gigante, I.; et al. Impaired bone remodeling in children with osteogenesis imperfecta treated and untreated with bisphosphonates: The role of DKK1, RANKL, and TNF-α. Osteoporos. Int. 2016, 27, 2355–2365. [Google Scholar] [CrossRef]
- Giordano, P.; Brunetti, G.; Lassandro, G.; Notarangelo, L.D.; Luciani, M.; Mura, R.M.; Lazzareschi, I.; Santagostino, E.; Piacente, L.; Ventura, A.; et al. High serum sclerostin levels in children with haemophilia A. Br. J. Haematol. 2016, 172, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Pouresmaeili, F.; Kamalidehghan, B.; Kamarehei, M.; Goh, Y.M. A comprehensive overview on osteoporosis and its risk factors. Ther. Clin. Risk Manag. 2018, 14, 2029–2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura, A.; Brunetti, G.; Colucci, S.; Oranger, A.; Ladisa, F.; Cavallo, L.; Grano, M.; Faienza, M.F. Glucocorticoid-induced osteoporosis in children with 21-hydroxylase deficiency. Biomed. Res. Int. 2013, 2013, 250462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, C.H.; Robling, A.G. Designing exercise regimens to increase bone strength. Exerc. Sport. Sci. Rev. 2003, 3, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Lassandro, G.; Palmieri, V.V.; Palladino, V.; Accettura, D.; Valente, R.; Giordano, P. Sport and Children with Immune Thrombocytopenia: Never Give up. Curr. Sports Med. Rep. 2019, 18, 317–318. [Google Scholar] [CrossRef]
- Lassandro, G.; Pastore, C.; Amoruso, A.; Accettura, D.; Giordano, P. Sport and Hemophilia in Italy: An Obstacle Course. Curr. Sports Med. Rep. 2018, 17, 230–231. [Google Scholar] [CrossRef]
- Lombardi, G.; Ziemann, E.; Banfi, G. Physical Activity and Bone Health: What Is the Role of Immune System? A Narrative Review of the Third Way. Front. Endocrinol. 2019, 7, 10–60. [Google Scholar] [CrossRef] [Green Version]
- Gardinier, J.D.; Al-Omaishi, S.; Morris, M.D.; Kohn, D.H. PTH signaling mediates perilacunar remodeling during exercise. Matrix Biol. 2016, 52–54, 162–175. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Onal, M.; Jilka, R.L.; Weinstein, R.S.; Manolagas, S.C.; O’Brien, C.A. Matrix-embedded cells control osteoclast formation. Nat. Med. 2011, 17, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- David, V.; Martin, A.; Lafage-Proust, M.H.; Malaval, L.; Peyroche, S.; Jones, D.B.; Vico, L.; Guignandon, A. Mechanical loading down-regulates peroxisome proliferator-activated receptor gamma in bone marrow stromal cells and favors osteoblastogenesis at the expense of adipogenesis. Endocrinology 2007, 148, 2553–2562. [Google Scholar] [CrossRef]
- Allen, J.; Sun, Y.; Woods, J.A. Exercise and the Regulation of Inflammatory Responses. Prog. Mol. Biol. Transl. Sci. 2015, 135, 337–354. [Google Scholar] [PubMed]
- Colaianni, G.; Grano, M. Role of Irisin on the bone-muscle functional unit. Bonekey Rep. 2015, 23, 4–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Valverde, P.; Zhu, X.; Murray, D.; Wu, Y.; Yu, L.; Jiang, H.; Dard, M.M.; Huang, J.; Xu, Z.; et al. Exercise-induced irisin in bone and systemic irisin administration reveal new regulatory mechanisms of bone metabolism. Bone Res. 2017, 5, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elizondo-Montemayor, L.; Mendoza-Lara, G.; Gutierrez-DelBosque, G.; Peschard-Franco, M.; Nieblas, B.; Garcia-Rivas, G. Relationship of Circulating Irisin with Body Composition, Physical Activity, and Cardiovascular and Metabolic Disorders in the Pediatric Population. Int. J. Mol. Sci. 2018, 19, 3727. [Google Scholar] [CrossRef] [Green Version]
- Colaianni, G.; Faienza, M.F.; Sanesi, L.; Brunetti, G.; Pignataro, P.; Lippo, L.; Bortolotti, S.; Storlino, G.; Piacente, L.; D’Amato, G.; et al. Irisin serum levels are positively correlated with bone mineral status in a population of healthy children. Pediatr. Res. 2019, 85, 484–488. [Google Scholar] [CrossRef]
- Faienza, M.F.; Brunetti, G.; Sanesi, L.; Colaianni, G.; Celi, M.; Piacente, L.; D’Amato, G.; Schipani, E.; Colucci, S.; Grano, M. High irisin levels are associated with better glycemic control and bone health in children with Type 1 diabetes. Diabetes Res. Clin. Pract. 2018, 141, 10–17. [Google Scholar] [CrossRef]
- Brunetti, G.; D’Amelio, P.; Wasniewska, M.; Mori, G.; Faienza, M.F. Editorial: Bone: Endocrine Target and Organ. Front. Endocrinol. 2017, 19, 8–354. [Google Scholar] [CrossRef] [Green Version]
- Faienza, M.F.; Chiarito, M.; D’amato, G.; Colaianni, G.; Colucci, S.; Grano, M.; Brunetti, G. Monoclonal antibodies for treating osteoporosis. Expert Opin. Biol. Ther. 2018, 18, 149–157. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef]
- Nimmo, M.A.; Leggate, M.; Viana, J.L.; King, J.A. The Effect of Physical Activity on Mediators of Inflammation. Diabetes Obes. Metab. 2013, 15, 51–60. [Google Scholar] [CrossRef]
- Mezil, Y.A.; Allison, D.; Kish, K.; Ditor, D.; Ward, W.E.; Tsiani, E.; Klentrou, P. Response of Bone Turnover Markers and Cytokines to High-Intensity Low-Impact Exercise. Med. Sci. Sports Exerc. 2015, 47, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- Govindaraju, D.; Atzmon, G.; Barzilai, N. Genetics, lifestyle and longevity: Lessons from centenarians. Appl. Transl. Genom. 2015, 4, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, L.; Elliott-Sale, K.J.; Sale, C. Exercise and bone health across the lifespan. Biogerontology 2017, 18, 931–946. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, K.; Nojiri, H.; Saita, Y.; Morikawa, D.; Ozawa, Y.; Watanabe, K.; Koike, M.; Asou, Y.; Shirasawa, T.; Yokote, K.; et al. Mitochondrial superoxide in osteocytes perturbs canalicular networks in the setting of age-related osteoporosis. Sci. Rep. 2015, 5, 9148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manolagas, S.C. From Estrogen-Centric to Aging and Oxidative Stress: A Revised Perspective of the Pathogenesis of Osteoporosis. Endocr. Rev. 2010, 31, 266–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrogini, E.; Almeida, M.; Martin-Millan, M.; Paik, J.H.; DePinho, R.A.; Han, L.; Goellner, J.; Weinstein, R.S.; Jilka, R.L.; O’Brien, C.A.; et al. FoxO-mediated defense against oxidative stress in osteoblasts is indispensable for skeletal homeostasis in mice. Cell Metab. 2010, 11, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Case, N.; Thomas, J.; Xie, Z.; Sen, B.; Styner, M.; Rowe, D.; Rubin, J. Mechanical input restrains PPARγ2 expression and action to preserve mesenchymal stem cell multipotentiality. Bone 2013, 52, 454–464. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, H.; Moreira-Gonçalves, D.; Esteves, J.L.S.; Viriato, N.; Vaz, M.; Mota, M.P.; Duarte, J.A. Voluntary exercise has long-term in vivo protective effects on osteocyte viability and bone strength following ovariectomy. Calcif. Tissue Int. 2011, 88, 443–454. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Loenneke, J.P.; Blackburn, E.H. Movement-Based Behaviors and Leukocyte Telomere Length among US Adults. Med. Sci. Sports Exerc. 2015, 47, 2347–2352. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, K.M.; Erik Rosengren, B. Physical Activity as a Strategy to Reduce the Risk of Osteoporosis and Fragility Fractures. Int. J. Endocrinol. Metab. 2012, 10, 527–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ertek, S.; Cicero, A. State of the art paper impact of physical activity on inflammation: Effects on cardiovascular disease risk and other inflammatory conditions. Arch. Med. Sci. 2012, 5, 794–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segev, D.; Hellerstein, D.; Dunsky, A. Physical Activity-does it Really Increase Bone Density in Postmenopausal Women? A Review of Articles Published between 2001–2016. Curr. Aging Sci. 2018, 11, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Gabel, L.; Macdonald, H.M.; Nettlefold, L.; McKay, H.A. Physical Activity, Sedentary Time, and Bone Strength from Childhood to Early Adulthood: A Mixed Longitudinal HR-pQCT study. J. Bone Miner. Res. 2017, 32, 1525–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, J.A.; Chesi, A.; Elci, O.; McCormack, S.E.; Roy, S.M.; Kalkwarf, H.J.; Lappe, J.M.; Gilsanz, V.; Oberfield, S.E.; Shepherd, J.A.; et al. Physical Activity Benefits the Skeleton of Children Genetically Predisposed to Lower Bone Density in Adulthood. J. Bone Miner. Res. 2016, 31, 1504–1512. [Google Scholar] [CrossRef] [Green Version]
- Ireland, A.; Muthuri, S.; Rittweger, J.; Adams, J.E.; Ward, K.A.; Kuh, D.; Cooper, R. Later Age at Onset of Independent Walking Is Associated with Lower Bone Strength at Fracture-Prone Sites in Older Men. J. Bone Miner. Res. 2017, 32, 1209–1217. [Google Scholar] [CrossRef]
- Tan, V.P.S.; Macdonald, H.M.; Kim, S.; Nettlefold, L.; Gabel, L.; Ashe, M.C.; McKay, H.A. Influence of physical activity on bone strength in children and adolescents: A systematic review and narrative synthesis. J. Bone Miner. Res. 2014, 29, 2161–2181. [Google Scholar] [CrossRef]
- Janz, K.F.; Letuchy, E.M.; Eichenberger Gilmore, J.M.; Burns, T.L.; Torner, J.C.; Willing, M.C.; Levy, S.M. Early physical activity provides sustained bone health benefits later in childhood. Med. Sci. Sports Exerc. 2010, 42, 1072–1078. [Google Scholar] [CrossRef] [Green Version]
- Going, S.B.; Farr, J.N. Exercise and Bone Macro-architecture: Is Childhood a Window of Opportunity for Osteoporosis Prevention? Int. J. Body Compos. Res. 2010, 8, 1–9. [Google Scholar]
- Bellew, J.W.; Gehrig, L. A comparison of bone mineral density in adolescent female swimmers, soccer players, and weight lifters. Pediatr. Phys. Ther. 2006, 18, 19–22. [Google Scholar] [CrossRef]
- Meyer, U.; Ernst, D.; Zahner, L.; Schindler, C.; Puder, J.J.; Kraenzlin, M.; Rizzoli, R.; Kriemler, S. 3-Year follow-up results of bone mineral content and density after a school-based physical activity randomized intervention trial. Bone 2013, 55, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, R.K.; Bauer, J.J.; Snow, C.M. Jumping Improves Hip and Lumbar Spine Bone Mass in Prepubescent Children: A Randomized Controlled Trial. J. Bone Miner. Res. 2001, 16, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.C.; Teixeira, A.S.; Goldberg, T.B.L. Sport and its implications on the bone health of adolescent athletes. Rev. Bras. Med. Esporte 2003, 9, 426–432. [Google Scholar] [CrossRef]
- Loud, K.J.; Gordon, C.M.; Micheli, L.J.; Field, A.E. Correlates of stress fractures among preadolescent and adolescent girls. Pediatrics 2005, 115, e399–e406. [Google Scholar] [CrossRef] [Green Version]
- Laing, E.M.; Wilson, A.R.; Modlesky, C.M.; O’Connor, P.J.; Hall, D.B.; Lewis, R.D. Initial years of recreational artistic gymnastics training improves lumbar spine bone mineral accrual in 4- to 8-year-old females. J. Bone Miner. Res. 2005, 20, 509–519. [Google Scholar] [CrossRef] [Green Version]
- McKay, H.A.; MacLean, L.; Petit, M.; MacKelvie-O’Brien, K.; Janssen, P.; Beck, T.; Khan, K.M. “Bounce at the Bell”: A novel program of short bouts of exercise improves proximal of femur bone mass in early pubertal children. Br. J. Sports Med. 2005, 39, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Hervás, G.; Ruiz-Litago, F.; Irazusta, J.; Irazusta, A.; Sanz, B.; Gil-Goikouria, J.; Fraile-Bermudez, A.B.; Pérez-Rodrigo, C.; Zarrazquin, I. Bone Health and Its Relationship with Impact Loading and the Continuity of Physical Activity throughout School Periods. Int. J. Environ. Res. Public. Health 2019, 8, 2834. [Google Scholar] [CrossRef] [Green Version]
- Boreham, C.A.G.; McKay, H.A. Physical activity in childhood and bone health. Br. J. Sports Med. 2011, 45, 877–879. [Google Scholar] [CrossRef]
- Sanchis-Moysi, J.; Dorado, C.; Olmedillas, H.; Serrano-Sanchez, J.A.; Calbet, J.A. Bone mass in prepubertal tennis players. Int. J. Sports Med. 2010, 31, 416–420. [Google Scholar] [CrossRef]
- Vlachopoulos, D.; Barker, A.R.; Ubago-Guisado, E.; Ortega, F.B.; Krustrup, P.; Metcalf, B.; Castro Pinero, J.; Ruiz, J.R.; Knapp, K.M.; Williams, C.A.; et al. The effect of 12-month participation in osteogenic and non-osteogenic sports on bone development in adolescent male athletes. The PRO-BONE study. J. Sci. Med. Sport 2018, 21, 404–409. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, D.; Barker, A.R.; Williams, C.A.; Knapp, K.M.; Metcalf, B.S.; Gracia-Marco, L. Effect of a program of short bouts of exercise on bone health in adolescents involved in different sports: The PRO-BONE study protocol. BMC Public Health 2015, 15, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, V.H. School-based exercise interventions effectively increase bone mineralization in children and adolescents. Osteoporos. Sarcopenia 2018, 4, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Zulfarina, M.S.; Sharkawi, A.M.; Aqilah-S.N, Z.-S.; Mokhtar, S.-A.; Nazrun, S.A.; Naina-Mohamed, I. Influence of Adolescents’ Physical Activity on Bone Mineral Acquisition: A Systematic Review Article. Iran. J. Public Health 2016, 45, 1545–1557. [Google Scholar] [PubMed]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faienza, M.F.; Lassandro, G.; Chiarito, M.; Valente, F.; Ciaccia, L.; Giordano, P. How Physical Activity across the Lifespan Can Reduce the Impact of Bone Ageing: A Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 1862. https://doi.org/10.3390/ijerph17061862
Faienza MF, Lassandro G, Chiarito M, Valente F, Ciaccia L, Giordano P. How Physical Activity across the Lifespan Can Reduce the Impact of Bone Ageing: A Literature Review. International Journal of Environmental Research and Public Health. 2020; 17(6):1862. https://doi.org/10.3390/ijerph17061862
Chicago/Turabian StyleFaienza, Maria Felicia, Giuseppe Lassandro, Mariangela Chiarito, Federica Valente, Loredana Ciaccia, and Paola Giordano. 2020. "How Physical Activity across the Lifespan Can Reduce the Impact of Bone Ageing: A Literature Review" International Journal of Environmental Research and Public Health 17, no. 6: 1862. https://doi.org/10.3390/ijerph17061862