Article Text

Abstract
Early identification of patients with sepsis is key to the delivery of the sepsis 6 bundle including antibiotic therapy within an hour.[1-3] Demand versus capacity challenges in the Emergency Department (ED) led to delays in antibiotic and sepsis 6 delivery. An alerting tool was developed that provided criteria for Scottish Ambulance Service (SAS) Paramedics to alert the ED of potential sepsis patients.
Data from patients presenting to the ED prior to the alerting process commencing (n=50) and during alerting (n=50) were analysed, a questionnaire was used to ascertain feedback from all staff groups; nurses doctors, and paramedics (n=38). Mean Time to triage improved by 82% from 17 minutes to 3 minutes (p=0.01), time to first antibiotic improved by 39% from 49 minutes to 30 minutes. Overall 78% of patients received antibiotics within an hour of leaving their home; no significant increase in workload was reported by staff.
In conclusion alerting by paramedics of potential sepsis patients reduced the time taken to deliver the Sepsis 6 Bundle. Process reliability has been sustained over several months. This process has been spread to seven regional ambulance stations in Lanarkshire Scotland.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Wishaw General Hospital is a district general hospital in Lanarkshire, Scotland. The Emergency Department (ED) sees 70,000 patients per year. Wishaw hospital is served by the West of Scotland SAS.
A problem was highlighted with the early identification and treatment of septic patients. This was felt to be due to increased activity and demand versus capacity in the busy ED. The cause of the problem was supported by data from the multidisciplinary ED sepsis team; the mean time to Triage for sepsis patients was 17 minutes, time to antibiotics was 49 minutes, and reliability of the sepsis 6 bundle was 78% (aim was 95% reliability). The mean time to triage of 17 minutes was therefore consuming nearly a third of the 60 minute timeframe for the delivery of the sepsis 6 care bundle.
Discussion at Lanarkshire's Sepsis Collaborative identified early recognition of sepsis as essential for the timely delivery of the sepsis 6 bundle, an issue also supported by the literature.1 ,2 The issue was shared with the ED staff and discussed at length. SAS were subsequently contacted to discuss the project. A small improvement team including consultant nurse, consultant ED physician, SAS paramedic, and SAS management team was established. The project team liaised and provided feedback to the multidisciplinary site team at the weekly ED sepsis meet.
The aim of this project was to demonstrate a 20% improvement in the time taken to identify potentially septic patients (as measured by the time to triage) and treat them (as measured by the time to antibiotics) within 12 months, through SAS Paramedics pre-alerting the ED of potentially septic patients. The time of arrival in the ED is taken as the start time for measurement of time to antibiotics.
Background
NHS Lanarkshire committed to the Scottish Patient Safety Programme (SPSP) sepsis work stream in 2012. In the two years that followed, NHS Lanarkshire developed multidisciplinary sepsis pilot teams in three EDs across three district general hospitals.3 The model for improvement was used to test improvements with Plan Do Study Act (PDSA) cycles aimed at implementing and improving the delivery of the sepsis 6 care bundle.
Sepsis causes significant morbidity and mortality as much as 35% in severe sepsis.4 Financial costs were estimated in the US at $16 billion per annum in 2001 and reported to be rising in 2007.5 ,6 Data from a multicentre European prospective observation study (SOAP Study) was used to estimate the cost of each case of sepsis at €25,000.7 Taking into account the UK sepsis prevalence this has been reported as equating to about £2 billion annually for the UK.8
The epidemiology of sepsis was more recently estimated in a review in 2012 and suggested the incidence of sepsis is significant with severe sepsis estimated to be as much as 300 cases per 100 000, with mortality estimated at 30% for sepsis, 50% for severe sepsis, and as much as 80% for septic shock.9 However, the data as reported was from developed countries.
The mortality rate of severe sepsis and septic shock is also significantly higher than other time-sensitive diseases. This has been reported as sepsis patients having a level of risk of mortality 6–10 times greater than if admitted with an acute myocardial infarction and 4–5 times greater than an acute stroke.10
There is compelling evidence that the implementation of the sepsis treatment bundle (sepsis 6) within the first hour of the recognition of severe sepsis (organ dysfunction) can markedly reduce mortality, in some studies by as much as 50%, with the number needed to treat reported at 4.6. The sepsis 6 is a care bundle that is based on the recommendations from the surviving sepsis campaign (SSC) but it simplifies the pathways in order to improve reliable delivery and subsequently patient outcome.11 ,12 The SSC bundle includes the administration of high flow oxygen, rapid intravenous fluid administration, and antibiotic administration together with blood cultures, lactate and haemoglobin, and urinary output assessment.12
The importance of early administration of antibiotics was highlighted by a study by Kumar and colleagues in 2006, who demonstrated that for every one hour delay in the administration of antibiotics in severe sepsis, the risk of death increases by 7.6%.13 The reduction in mortality from sepsis has been the focus of worldwide and national campaigns, namely the SSC and now SPSP.3 ,12
However, a recent systematic review and meta-analysis of literature looked at the timing of antibiotic administration and outcome in severe sepsis and sepsis shock. The reviewers found no benefit in mortality based on administration of antibiotics within three hours of ED triage or within one hour of shock recognition in severe sepsis and septic shock. They concluded that time to antibiotics should not be used as a measure of quality of care. The reviewers did however “recognize that failure to administer effective antimicrobial therapy will at some time point be detrimental to patient outcomes, the exact time frame when this shift begins to occur remains unknown”.14
Sepsis has very recently been “redefined” by the third international consensus group, “As a life-threatening organ dysfunction caused by a dysregulated host response to infection” with the recommendation to implement Sequential (Sepsis related) Organ Failure Assessment (SOFA) for assessment causing significant debate.15
With the support of the SPSP programme, NHS Lanarkshire sepsis pilot teams had defined severe sepsis as a Systemic inflammatory Response Syndrome (SIRS) score of 2 or more, with evidence of probable infection and a Modified Early Warning Score (MEWS) of 4 or greater.16 The MEWS trigger of 4 was derived from Daniels and colleagues study who reported patients median MEWS at time zero of 6.0 (range 0-15), with n=467 (81.2%) of patients meeting the trigger threshold of 4.11
The activation of SIRS is a physiological response in the presence of inflammation, often accompanied by infection, but not exclusively so. SIRS criteria alone lacks sensitivity of detecting sepsis and should be used in conjunction with a severity score, in our case MEWS.11
The SIRS criteria tested were respirations >20, pulse >90, temp >38.5 or <36, WBC >12 or <4, blood glucose of >7.7 in absence of diabetes and reduced conscious level with the removal of WBC criteria due to potential time delay in obtaining results in the ED. These criteria were key to the development and testing of the paramedic pre alerting tool for suspected sepsis patients. The UK Sepsis Trust pre hospital recommendation and pre hospital screening tool were also taken into consideration prior to testing.17
An increased incidence of severe sepsis presentations to ED has been reported internationally, in comparison with acute myocardial infarction and stroke.2 Moreover the study highlights the pre-hospital interval as an important opportunity for recognition of sepsis due to its time sensitive nature.2 In relation to Scotland, one study reported that approximated 88% of patients with severe sepsis present to Scottish ED's by ambulance.1
There is a lack of publications on the design, testing, and efficacy of pre hospital sepsis alert tools used to alert EDs of suspected sepsis patients. With this in mind and with evidence to support the time sensitivity of treating severe sepsis the pre alerting of suspected cases was the focus for this improvement project.
Baseline measurement
The ED is a busy environment for staff with not only increasing acuity and an aging patient population, but also national and regional targets including triage time, waiting time, and patient flow identified as areas for improvement.
Review of reliability of the delivery of the sepsis 6 bundle within the ED based on 50 patients, led the team to identify time to triage (mean 17 minutes), time to antibiotic (mean 49 minutes) and sepsis 6 reliability of 78% as an opportunity for improvement. Time zero (time when clock started for sepsis delivery within 1 hour) was operationally defined as the time sepsis was identified. In all cases this equated to the time the patient “booked into” the ED, for SAS patients.
Triage time was highlighted as the primary target area for improvement. The team hypothesised that if suspected sepsis patients were pre alerted then this would subsequently reduce/eliminate triage and reduce the time to antibiotics and sepsis 6 delivery. The aim was to improve these measurements by 20% in a 12 month period.
The data below were included in the project measurement plan. The team analysed data from SAS septic patients prior to the implementation of the Alerting process (n=50) and during the alerting process (n=50). Data were extracted retrospectively from case note review, recorded by hand and later transcribed onto excel for analysis. All data were checked for accuracy and then quality assured by the consultant ED physician. The improvement project measurements were; the time from the SAS alert call to the arrival at the ED; the time of triage; the time to first antibiotic dose; the time to sepsis 6 completion (all components of the bundle delivered) and the percentage of patients who had Sepsis 6 completed within 60 min. Furthermore, the number of “false” sepsis alerts (alerted patients who were diagnosed as not sepsis by the ED) was also noted.
Staff concerns regarding a potential increase in workload were noted. To assess this, a questionnaire was constructed to gauge staff feedback (See Supplementary File SAS Tool and Questionaire). This was identified as a possible balancing measure (increased workload).
The questions were developed from themes noted during staff discussions. The themes were then refined following results from a test of the questionnaire. ED nurses, senior doctors, and paramedics not directly involved in the alerting process were asked how appropriate they felt the responses were.18 The questionnaire was in written format; participation was voluntary and responses anonymised. The questionnaire was circulated to all staff groups during the alerting phase of the project.
Statistical analysis was conducted by using a t test to test for differences in mean time to triage for both groups i.e. prior introduction of the alerting process and during the alerting process.
Design
With evidence to suggest that 88% of septic patients arrive by ambulance, pre alerting of septic patients was highlighted as a key area for improvement in time to deliver the sepsis 6.1
The first step in the improvement design was to engage key stakeholders, namely ED staff, who were already involved in hospital testing and SAS leaders with a view to forming a small improvement team. This was done by presenting the ED baseline data together with the background on sepsis, sepsis mortality, and the sepsis 6 treatment pathway to key SAS leaders. A series of meetings were used to highlight the potential impact of a proposed pre alerting process for suspected sepsis patients and the impact on patient outcome. A local SAS station was carefully chosen to design and test a draft alerting process.
The next step was to work with the paramedics in the field as they treated patients in order to observe their processes and systems. The consultant nurse worked with one paramedic at one station in order to learn their ways of working.
The final step was to commence the design of a simple tool that would take into account the paramedics and ED current processes. A simple tool was then designed by the team. (See Supplementary File SAS Tool and Questionaire) The tool was then tested and refined through multiple PDSAs, the tool for testing included source of infection, vital signs, and patient allergies. Paramedics called the ED with this information. By pre-alerting the department of potentially septic patients, the department would prioritise these patients, seeing them as soon as they arrived. The ED staff prepared for the patients arrival with the belief that this would reduce time to triage and instigation of the sepsis 6 treatment bundle.
Using the Model for Improvement, training for this tool was undertaken with a Paramedic on a 1-1 basis. Further PDSAs refined the alerting process over the next two months. Paramedics and the ED team were fully involved in providing feedback at weekly ED sepsis meetings in an effort to further improve the process. Additional PDSA cycles were completed to spread the process over a testing period of four months and included all paramedics at one testing SAS station. Educational support included 1:1 sepsis sessions that provided a brief overview of pathophysiology, incidence, mortality, and treatment, with particular emphasis placed upon the time sensitive aspects of the sepsis 6 care bundle.
Strategy
The Model for Improvement with multiple PDSA cycles were used to observe practice, design, and then test the paramedic sepsis alerting tool. (Details of the PDSA cycles are shown in the Supplementary File PDSA)
PDSA 1
Tested if the pre alerting process could be used by paramedics for suspected sepsis patients.
PDSA 2
Tested a call to the ED stand by phone using the refined Alerting tool.
PDSA 3
Tested a statement of “Sepsis pre alert call” test instead of “Stand by” call.
Initial plans were to deliver intravenous antibiotics to patients by the paramedics at the scene with radio communication providing professional to professional support. This was rejected for testing as it was felt to be overly complex, impractical, and unnecessary for the majority of the geographical locations of sepsis calls received by the testing SAS station.
PDSA cycle 1 tested the concept that a pre alerting process could be used by paramedics for sepsis patients. We learned that vital signs were recorded reliably but, due to nature of pre-hospital working methods and time constraints the National Early Warning Scores (NEWS) was usually calculated retrospectively. Observational sessions provided invaluable insight, facilitated the development of the teams to improve the process and helped with essential team building. We concluded we could test SIRS, vital signs, and source of infection in a pre alert tool with the only additional workload being the radio call to the ED.
The paramedic, nurse consultant, and ED consultant then progressed to design a draft alerting tool that focused on the above patient information. The process was then tested by a single paramedic. Initial feedback from ED staff and the paramedic was positive, but the radio call was highlighted as an issue.
PDSA cycle 2 tested a call to the ED stand by phone using the refined Alerting tool. Following suggestion from ED consultant the PDSA added “Patient Allergies” to the tool. Feedback was positive but noted potential for misunderstanding i.e. was this a “stand by” call.
PDSA cycle 3 included a statement of “Sepsis pre alert call” test instead of “Stand by” call this was clearly understood by staff. Feedback was positive and prompted staff to think about good antimicrobial stewardship.
The alerting process was then spread gradually by providing 1:1 teaching sessions to 3, then 5, then all 10 paramedics at one station.
Results
Of those alerted patients, n=43 (86%) had a MEWS of 4 or more, and met the inclusion criteria for our definition of severe sepsis. Sources of infection for alerted patients were chest sepsis n=36 (72%), urinary sepsis n=9(18%), chest and urine sepsis n=1 (2%), neutropenia 1 (2%), and unknown origin n=3 (6%). Non septic patients or those with significant data missing were excluded as where patients alerted by “inadvertent spread” to non testing stations.
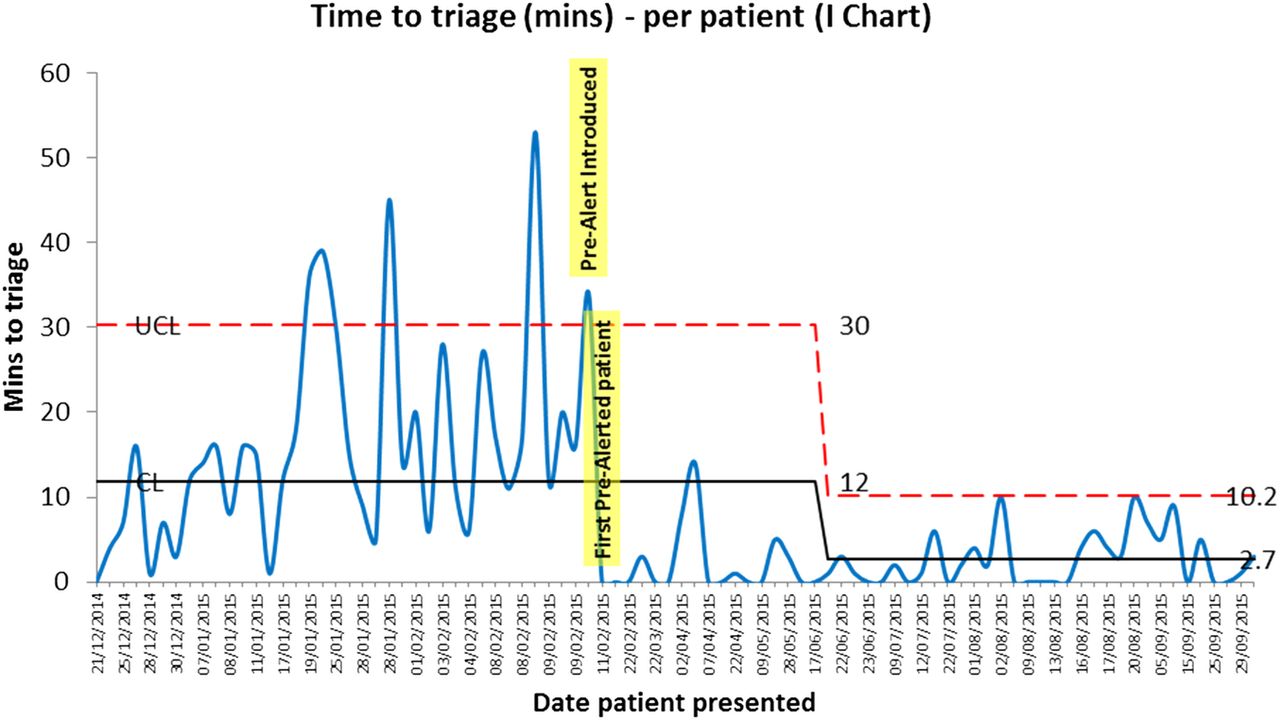
Triage times for non-alerted (n=50) and alerted (n=50) sepsis patients are illustrated in Figure 1. Time to Triage is used as a surrogate for the time taken to identify potentially septic patients and was reduced by 82% (17 minutes to 3 minutes) with a reduction in process variation noted. The reduction in the variation is indicative of the introduction of the alerting tool and subsequent standardisation of the process afterwards. A t test showed statistical difference between alerted and non alerted mean times to triage, p=0.01.
{kind=link}
Time to Triage in minutes per patient
Time to antibiotic improved by 39% (49 minutes to 30 minutes) which indicates a reduction in the time to treatment. Overall, the sepsis 6 process reliability (percentage of patients successfully receiving the complete bundle within 60 minutes) improved from 78% to 98%. Importantly it was noted that 78% of pre alerted patients received the sepsis 6 bundle within an hour of leaving home.
Balancing measures included results from a staff questionnaire. The questionnaire focused most notably on the degree of workload as perceived from the multidisciplinary team (n=38), doctors (n=14), and nurses (n= 18) in the ED and SAS paramedics (n=6). No significant increase in workload was reported by any staff group with 89% (n=34) reporting that the alerting process improved care for sepsis patients.
Further balancing measures were evaluated via the number of “False positives”; the alerting of non-sepsis patients. These were minimal and decreased over time with ED staff reporting simple step down for these patients.
Lessons and limitations
A number of important lessons were learned during this project. Firstly the importance of multidisciplinary team work. One key example of this was the valuable learning gained from observing SAS colleagues in the field in order to understand their way of working. This informed the design of the alerting process. The decision to build the tool around the actual process of the SAS paramedics routine working pattern was essential.
Secondly the decisions to keep the tool very simple and resist the temptation to add to it or overcomplicate it. This decision was informed again by the early learning in the project from the paramedics.
Thirdly the value of real time feedback and open discussion and debate, at weekly meetings of the NHS Lanarkshire's reducing harm collaborative. This regional approach allowed the team to share experiences, data, and learning as well as facilitating education for colleagues in other neighbouring ED's.
Additionally, the decision to form a small improvement team was also crucial. This allowed quick and simple decision making that was based on real time data from testing. These data were then used to feedback to the wider ED staff and SAS colleagues in order to build will and improve team rapport. Overall this helped with the embedding and the subsequent ownership of the process as well as longer term process reliability and sustainability. Building on from this we have spread to include seven SAS stations whilst maintaining > 95% reliability of sepsis 6 process.
Finally the decisions to resist accelerated spread early in the project allowed the improvement team time to build will with a few colleagues who feared over alerting and alert fatigue. We managed to overcome this challenge as more supporting data and patient stories became available.
Challenges included potential alert fatigue, namely potential to underestimate incoming sepsis alerts due to the volume of calls for all ED alerts, such as myocardial infarction and stroke, or desensitisation of the process. This was addressed by weekly review of all SAS alerted cases, feedback and discussion and sharing of process reliability data with the ED and SAS staff.
This study was not designed to change the time taken to assess the patients. This remained constant throughout the study period. During this ~25 minute period, the patient received initial medical and nursing assessments, monitoring, IV access and the other components of the Sepsis 6 bundle required before safely delivering antibiotic therapy.
Limitations of the project included inadvertent spread by SAS paramedics into SAS stations that were not formally testing the process. This may have resulted in some bias. Although they were effective in alerting some patients, the process was not underpinned by teaching or supported by the improvement methodology. To minimise the potential for bias from this source, these data were removed from the project analysis. This inadvertent spread may have been reduced by more effective and consistent communication by the improvement team.
Other potential limitations to the generalisability of this study's findings may be that the geographical location of the SAS stations was in relative close proximity to the test ED. The recorded SAS travel time to hospital was for most patients less than 15 minutes, but a few patients took up to 25 minutes. The process described for pre-alerting of patients with a greater travelling time to the ED would still be applicable, however possible on site treatment for severe sepsis with antibiotic delivery should be tested.
Conclusion
The introduction and sustained use of the alerting tool by paramedics has improved the time to triage and thus time to antibiotic and time to sepsis 6 for patients presenting with sepsis by ambulance. Reducing time to triage coupled with pre identification of suspected sepsis patients has provided valuable minutes required to meet the sepsis 6 delivery within 60 minutes.
To our knowledge, there have been no high quality studies specifically looking at the benefits from pre-hospital identification or alerting processes. It has been suggested that work needs to be done to look at this area.19
The team approach facilitated by the sepsis collaborative has helped embed ownership of the process with regular review and feedback helping to refine the process.
The reliability of the alerting process has been sustained. The alerting process has now been spread to seven SAS stations. The spread plan to these and other SAS stations has been subject to careful but deliberate debate and based data and staff feedback specifically in relation to workload.
We continue to monitor its use and the efficacy of the process. We are working with colleagues to share our learning from this project and the integration of this work into the national agenda for SAS and pre hospital alerting.
Acknowledgments
Ann Rodger SAS, Andy Graham SAS, SCN Tracy Dodd ED, Wishaw Hospital ED staff and Hospital Emergency Care Team, Connie Sharrock, Joe Hands, Raymond Hamill, Ann Hair.
Footnotes
Declaration of interests None declared.
Ethical approval This project was exempt from ethics approval as it was deemed an improvement project as part of NHS Lanarkshire reducing harms collaborative.