
Abstract
Background
The population is aging globally. Older people living in long-term care facilities have many functional impairments, such as mobility problems and depression. Digital games and so-called exergames can offer a motivating and entertaining way to maintain older people’s physical activity and thus their ability to function. However, previous studies have reported conflicting results about the effects of digital gaming and have focused on community-dwelling older people.
Objective
To identify, critically appraise, and synthesize evidence about the effectiveness of digital games on older people’s physical, psychological, and social functioning and physical and social activity in long-term care facilities.
Methods
Five databases were systematically searched, and relevant studies were screened. Fifteen randomized-controlled trials and quasi-experimental studies (total N = 674) were included in meta-analysis.
Results
All digital games used in interventions were exergames. Meta-analysis showed that exergame interventions have a statistically significant large effect on physical functioning [number of studies (N) = 6, standardized mean difference (SMD) = 0.97, p = 0.001] measured by Timed Up and Go or Short Physical Performance Battery and self-assessed physical activity (N = 3, SMD = 1.20, p < 0.001) and medium effect on social functioning (N = 5, SMD = 0.74, p = 0.016) compared to alternative intervention or no intervention. Social activity was not measured in any study.
Conclusions
The results are encouraging that exergames effectively increase the functioning and activity of older adults living in long-term facilities. Successful implementation of such activities requires the competence of nursing staff and rehabilitation professionals in digitalization.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The population is aging globally, and the number of older people is estimated to more than double from 2020 to 2050, when 16% of the world’s population will be over 65 years old [1]. As the number of older people is growing, the number of people living in long-term care facilities is also increasing. Older people living in long-term care facilities are more likely to be functionally and cognitively impaired than their independent peers [2]. Living in long-term care facilities has been found to cause a decline in physical functioning [3], and it has also been found to result in experiencing symptoms of depression, loneliness, and social isolation in older people [2, 4].
The physical activity of older people is related to physical and psychological functioning and functional impairments [5, 6]. Exercise and even light physical activity have a positive effect on the physical functioning of older people and coping with activities of daily living (ADL) for older people living in assisted living facilities [7,8,9]. Physical activity has also been found to smooth out the worsening of depressive symptoms in care home residents [6]. Higher physical activity is also correlated with a higher quality of life of older people [10]. However, residents in long-term care environments have many barriers to physical activity, which can affect their motivation to exercise [11]. The fun, enjoyment, and sociability of training are big motivators for exercise among older people [12, 13], and digital games and exergaming enable these dimensions [14].
Digital games are games played on a digital device. A digital device can be, for example, a computer, a game console, a tablet computer, or a smartphone. According to previous reviews studying digital games, Nintendo Wii and Microsoft Kinect have been the most used gaming systems by older people [15]. Playing these kinds of active video games where the player uses one’s own body movement is often called exergaming [14]. Playing digital games that train balance, coordination, physical performance, and physical activity has been found to have a positive effect on the physical and psychological functioning of older people by reducing the experience of depression and improving balance. According to the previous studies, older people find digital games to be more motivating and entertaining than normal physical activities [16, 17]. Playing exergames is often social experience and it offers an opportunity for playfulness and social interaction [18]. This increased interaction with others during the play can decrease loneliness and strengthen social connection also among older people [18, 19]. Social isolation has been found to increase cognitive decline [20] and low cognitive skills hinder, among other things, older peoples’ coping with daily activities. There are already several systematic reviews about effects of exergaming on cognition of older adults that show the benefits of exergames having a positive influence on processing speed, working memory, and executive function [21].
Previous studies have also obtained conflicting results regarding the effects of digital gaming [22, 23]. The existing literature and earlier systematic reviews of digital gaming have focused on the home environment, and digital games have not been studied much in the long-term care environment [24]. More research is therefore needed on the effects of playing digital games on the functioning and activity of older people in long-term care.
The objective of this review was to identify, critically appraise, and synthesize evidence about the effectiveness of playing digital games on older people’s physical, psychological, and social functioning and physical and social activity in long-term care facilities. Two research questions were addressed:
-
1.
What digital gaming interventions have been conducted for older people in long-term care facilities?
-
2.
What is the effect of digital gaming versus usual care or conventional exercise on older people’s functioning and activity in long-term care facilities?
Methods
A systematic review and meta-analysis were conducted according to Joanna Briggs Institute guidelines [25]. The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement was applied for reporting the review [26]. The review was registered in PROSPERO (CRD42022307491). No protocol was published for this systematic review.
Search strategy
Data retrieval was carried out by an informant scientist. PubMed, Web of Science, CINAHL (EBSCO), Scopus, and Cochrane electronic databases were used to retrieve studies published up to November 2021. No publication period restrictions were made. Key Medical Subject Headings (MESH) terms and CINAHL headings were applied in the searches whenever possible. Search terms for research question one combined the following subject headings and keywords, formatted according to the requirements for each database: digital game, older people, and long-term care. Search terms for research question two combined the following subject headings and keywords, formatted according to the requirements for each database: digital game, older people, functioning, social activity, and physical activity. Synonyms were combined using the OR operator, and different search terms were combined using AND operator. NOT operator was used to exclude children and adolescents. The complete search terms for each database are presented in Appendix Table 4. A manual search was conducted in the reference lists of the articles included. No new references were found by manual searches.
Study selection and data extraction
Two reviewers (SK and either SE, SA, or HS) independently screened records for inclusion in the title and abstract phase and in the full-text phase. Selection was made based on the inclusion and exclusion criteria created according to the PICO format. Full-text original research articles were eligible. Study inclusion and exclusion criteria were as follows: older people without specific diseases excluding memory disorders living in long-term care (population), digital gaming interventions (intervention), control group with usual care or alternative intervention (comparator), and change in measured physical, psychological, or social functioning and/or change in physical or social activity from baseline to the last available follow-up (outcome). Studies measuring physical functioning using the Timed Up and Go (TUG) test or Short Physical Performance Battery (SPPB) were chosen for this review. These tests were chosen, because they measure a wide area of physical functioning, considering balance, strength, agility, and walking speed. The measures used for mental and social functioning and activity were not limited. Interventions that combined digital gaming with, for example, conventional exercise or physical therapy were not eligible. Only studies published in English were included due to the lack of resources for the translation of other languages. Reviewers were blinded to each other’s decisions and conflicts were solved in the consensus of two reviewers. If the consensus was not reached, a third reviewer was consulted. Data extraction was done by one researcher (SK), and another researcher (SE) checked the quantitative data. Data selection and extraction were done and recorded via Covidence systematic review software.
Quality assessment
A quality assessment was made for 15 studies that met the inclusion criteria in accordance with the quality assessment criteria of the Joanna Briggs Institute. Quality assessment was made by two independent reviewers (SK and either SE, SA, or HS). Disagreements were solved in the conclusion of two reviewers. Studies were accepted for the review if 50% of the assessment criteria were met. All 15 studies were accepted for the review. The quality assessment for RCT studies is presented in Table 1 and for quasi-experimental studies in Table 2.
1. Was true randomization used for the assignment of participants to treatment groups?
2. Was allocation to treatment groups concealed?
3. Were the treatment groups similar at the baseline?
4. Were participants blind to the treatment assignment?
5. Were those delivering treatment blind to the treatment assignment?
6. Were outcome assessors blind to the treatment assignment?
7. Were the treatment groups treated identically other than the intervention of interest?
8. Was follow-up completed, and if not, were differences between groups in terms of their follow-up adequately described and analyzed?
9. Were participants analyzed in the groups to which they were randomized?
10. Were outcomes measured in the same way for the treatment groups?
11. Were outcomes measured in a reliable way?
12. Was an appropriate statistical analysis used?
13. Was the trial design appropriate, and were any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial?
1. Is it clear in the study what is the ‘cause’ and what is the ‘effect’ (i.e., there is no confusion about which variable comes first)?
2. Were the participants included in any comparisons similar?
3. Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest?
4. Was there a control group?
5. Were there multiple measurements of the outcome both pre- and post-intervention/exposure?
6. Was follow-up complete, and if not, were differences between groups in terms of their follow-up adequately described and analyzed?
7. Were the outcomes of the participants included in any comparisons measured in the same way?
8. Were outcomes measured in a reliable way?
9. Was the appropriate statistical analysis used?
Data analysis and synthesis
Narrative synthesis and meta-analysis were conducted for all 15 studies. Separate meta-analyses were performed for RCT studies and quasi-experimental studies and for different outcomes. The level of statistical significance was p < 0.05. Post-intervention means and SD values of continuous outcomes were used to calculate standardized mean differences (SMD) and 95% confidence intervals (CIs) between groups with Cohen’s d value. If the study had multiple experimental or comparator groups, the best matching group was chosen for meta-analysis, usually the passive control group. Mean, standard deviations, and sample sizes were estimated when they were not directly reported. A random-effects model was used for the meta-analysis due to differences between interventions and populations. The effect size was considered small (SMD = 0.2 to 0.5), medium (SMD = 0.5 to 0.8), or large (SMD > 0.8). Statistical heterogeneity was observed with the Chi2 test and I2 test. The significance level of the Chi2 test was p < 0.10, indicating heterogeneity. In the I2 test, the value of 0–40% would be considered low heterogeneity, 30–60% indicates moderate heterogeneity, 50–90% indicates substantial heterogeneity, and 75–100% indicates considerable heterogeneity [27]. Publication bias could not be assessed with statistical methods due to the small number of studies per outcome.
Results
Search outcomes
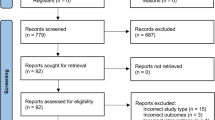
The search yielded 10,762 references, and after removing duplicates, 7429 references remained. Then, 139 full texts were assessed. A total of 124 studies were excluded, and 15 articles were included for the review. The search outcomes are shown in Fig. 1.

PRISMA flow diagram of the article selection process
Study characteristics
Studies selected for this review were conducted between 2009 and 2021 in Belgium [28, 29], The Netherlands [30], Spain [31], Turkey [32], The United Kingdom [33], Lebanon [34], Taiwan [35], Singapore [36], Iran [37], USA [38], Brazil [39, 40], South Africa [41], and Australia [42]. Six studies were RCTs [28, 29, 31, 33, 34, 37], and nine were quasi-experimental studies [30, 32, 35, 36, 38,39,40,41,42]. The sample sizes ranged from 19 to 106 participants (N = 674). The mean age of the study participants ranged from 66.5 to 87.5 years. In four studies, participants had cognitive disorders like memory complaints or Alzheimer’s disease [28, 29, 38, 41]. In one study, participants had poor balance [37]; in two studies, participants had frailty syndrome or risk for frailty syndrome [29, 39]; and in one study, all participants were women [40]. A summary of the participants, measures, intervention(s), control, and results is given in Table 3.
Risk of bias
The quality assessment points of the RCT studies ranged from 7 to 9 points (Table 1). Randomization was used in all six studies, but the concealment of allocation to treatment groups was unclear in all six studies. Blinding of participants and personnel was not possible due to the nature of the interventions. Outcome assessors were blinded in three studies [28, 29, 34]. The assessment point average was 8/11, so all RCT studies were of high methodological quality.
In quasi-experimental studies, assessment points ranged from 6 to 9 points (Table 2). The assessment point average was 7/9, indicating high methodological quality. In two studies, participants were not similar in the two groups due to gender [35] or function for activities of daily living [40]. In three studies, this assessment criteria was unclear, because participants’ characteristics were not presented clearly [36, 40, 42]. In five studies, follow-up was not complete and reasons for dropouts were unclear or the effect of dropouts on the results was not analyzed [30, 32, 39, 40, 42]. Randomization of participants was not done in quasi-experimental studies, and in three trials, participants chose the group they wanted to join [32, 35, 39].
Characteristics of the described interventions
All digital games used in the interventions were exergames. In six studies, the gaming console was Nintendo Wii [30, 32, 34, 36, 38, 42]. The Microsoft Xbox-360 Kinect console was used in four studies [35, 37, 40, 41]. In three studies, participants played exergames that utilized Kinect motion sensors. The games were FRED [31], SIRTET [39], and MIRA-system [33]. In two studies, games utilized a force platform to control games [28, 29]. These games were designed to improve, for example, balance, strength, and flexibility.
In three studies, participants were divided into three groups [30, 32, 37]. One study compared exergaming to conventional balance training and usual care [37], one to conventional exercise and usual care [32], and one compared experienced Wii players to inexperienced players and to usual care [30]. Twelve studies divided participants into two groups. In six studies, exergaming interventions were compared to usual care [28, 31, 34, 35, 39, 42]. Two studies compared exergaming to playing traditional games [36, 40]. Padala et al. [38] and Ramnath et al. [41] compared exergaming to conventional exercise. In one study, controls listened to favorite music [29], and in one study, they received standard community fall prevention advice and an exercise leaflet [33].
Interventions lasted from 3 to 12 weeks, with 8 and 12 weeks being the most popular ones. Participants played games from two to five times per week, and in most of the studies (8), participants played games three times per week. Gaming sessions lasted from 15 min to 1.5 h. In one study, participants selected the frequency, duration, and type of games [42]. In six interventions, participants played games individually [29, 31, 32, 38,39,40], in one intervention, games were played with a partner in a group of two pairs [41], in three interventions in group [30, 36, 42], and in one study individually or in a group [33]. Four studies did not report whether the games were played in a group or individually [28, 34, 35, 37].
Outcome measures
Physical functioning was measured by the TUG test and SPPB. Psychological functioning was measured by the Hamilton Rating Scale for Depression (HRSD), Beck Depression Inventory (BDI), Geriatric Depression Scale (GDS), and Cornell Scale for Depression in Dementia (CSDD). Social functioning was measured by the Word Health Organization Quality of Life short-form (WHOQOL-BREF) questionnaire and the quasi-HRQOL questionnaire. Only the social functioning domains of the quality-of-life questionnaire were included in this review. Loneliness was measured by the UCLA loneliness scale. Physical activity was measured by the Physical Activity Scale for the Elderly (PASE), Rapid Assessment of Physical Activity (RAPA), Physical Activity Questionnaire for Elderly Japanese, and the LASA Physical Activity Questionnaire (LAPAQ).
Effectiveness of interventions
Ten studies assessed changes in physical functioning measured by TUG [28, 32,33,34, 37,38,39, 41] or SPPB [29, 31]. Eight of the ten studies reported significant positive changes in TUG or SPPB scores in the exergame group [28, 29, 31, 32, 34, 37, 39, 41]. Five studies reported significant between-group changes in favor of exergaming compared to alternative intervention or control groups [29, 32, 34, 37, 41]. In three studies, physical functioning in the exergaming group improved and the control group did not, but those studies did not report between-group p values [28, 31, 39]. Two studies did not find statistically significant inter-group or between-group differences [33, 38].
Psychological functioning was measured in four studies using different depression scales [29, 32, 33, 40]. Three of the four studies reported a positive change in depression scale scores of the exergame group after intervention [29, 32, 40], while the alternative intervention group or control group did not improve. In Cicek et al. [32], the conventional exercise group scores improved, but the control group did not. Two studies reported significant between-group changes in favor of exergaming [29, 40].
Social functioning was measured in five studies [32, 35, 36, 40, 42]. In three studies, results in exergaming groups improved, but control/alternative intervention groups did not improve [35, 36, 40]. In Cicek et al. [32], exergaming group, conventional exercise group, and control group results improved, but the improvement was not statistically significant. Between-group comparison revealed that three studies had statistically significant differences between the experimental group and the alternative intervention group or control group in favor of exergaming [35, 36, 40].
Four studies measured changes in physical activity [30, 33, 36, 42]. All four studies reported increased levels of physical activity in exergaming groups, but in Stanmore et al. [33], the results were not statistically significant. In three studies, the exergame group improved more than the alternative intervention or control group in between-group comparison [30, 36, 42].
Meta-analysis
A meta-analysis was conducted on six RCT studies (number of individuals, n = 278) that investigated the effect of exergaming on physical functioning [28, 29, 31, 33, 34, 37]. A meta-analysis on pooled TUG and SPPB scores showed a large effect in favor of exergaming (SMD = 0.97, 95% CI [0.42, 1.52], p = 0.001). A meta-analysis was conducted on four quasi-experimental studies (n = 116) that investigated the effects of exergaming on physical functioning as measured by TUG [33, 38, 39, 41]. A meta-analysis of pooled TUG scores showed that there is no significant difference between exergaming and comparator groups (SMD = 0.34, 95% CI [0.17, 0.86], p = 0.19).
A meta-analysis was conducted on two RCT studies (n = 137) that investigated the effects of exergaming on depression [29, 33]. A meta-analysis of pooled depression scale scores showed that there is no significant difference between groups (SMD = 0.52, 95% CI [− 0.59, 1.63], p = 0.35). Another meta-analysis was conducted on two quasi-experimental studies (n = 40) that investigated the effects of exergaming on psychological functioning (depressive symptoms) [32, 40]. A meta-analysis of pooled depression scale scores showed that there is no significant difference between groups (SMD = 1.46, 95% CI [− 0.46, 3.38], p = 0.14).
A meta-analysis was conducted on five quasi-experimental studies (n = 192) that investigated the effects of exergaming on social functioning [32, 35, 36, 40, 42]. A meta-analysis of pooled quality-of-life social domain scores and loneliness scale scores showed a medium effect in favor of the exergaming group (SMD = 0.74, 95% CI [0.14, 1.35], p = 0.016).
A meta-analysis was conducted on three quasi-experimental studies (n = 91) that investigated the effects of exergaming on physical activity [30, 38, 42]. A meta-analysis of pooled physical activity scale scores showed a large effect in favor of exergaming (SMD = 1.20, 95% CI [0.74, 1.66], p < 0.001). The results of the meta-analysis are shown in Fig. 2.

Forest plot of pooled effect sizes of individual studies
Discussion
Based on the results of this review, exergaming has a positive effect on the physical functioning of long-term care residents measured by TUG or SPPB. In previous reviews, it has also been found that exergaming has a positive effect on the balance, mobility, and walking of older people [43,44,45]. Unlike in this review, those studies also included older people living at home and people who used gaming, for example, for rehabilitation of Parkinson’s disease. In a meta-analysis performed by Taylor et al. [22], there were no statistically significant differences in TUG scores when exergames were compared with no intervention or with conventional exercise. Based on the results of this review, exergaming seems to be effective in improving walking speed, lower limb muscle strength, and balance in older people with memory disorders [28, 29, 41], which supports the results of a previous study [46]. In studies where participants had already diagnosed frailty syndrome or poor balance, TUG scores improved after exergaming intervention. This finding is in line with the previous research [47].
Earlier research has reported mixed results regarding the effects of exergaming on older adults’ mood and depression. In Zeng et al. [47], exergaming did not affect the mood of older people, but in Yen & Chiu [48], exergaming had a large effect on older adults’ depression. In this review, results were also mixed. In three of four studies, depression scale scores were statistically significantly lower after exergaming intervention, indicating fewer symptoms of depression [29, 32, 40]. However, the meta-analysis of RCT studies or quasi-experimental studies comparing exergaming to alternative intervention or no intervention did not reach the limit of a statistically significant difference. Previously, exercising has been found to reduce the symptoms of depression in older people [49, 50]. Also, in this study, four out of five experimental groups doing physical exercises or playing exergames improved in depression scores, but among participants in physically passive intervention or control groups, the scores did not improve. Only four studies measured the effects of exergaming on depression, so this field needs more empirical research.
Social isolation has many adverse health effects, including a higher risk of mortality [51], so a variety of interventions have been implemented for older people to reduce loneliness and increase social interaction [52]. Playing exergames with a partner has been found to reduce loneliness of the older people [53]. In this current review, participants’ loneliness was measured only in one study, and in the other four studies, social functioning was measured as a part of the quality-of-life measurement. Vázquez et al. [54] also found that none of the studies included in their review focused on social health. However, their meta-analysis showed that participants in the exergame group experienced higher beneficial effects from video game-based interventions than those in the control group. In addition, Li et al. [19] summarized that exergames could be an effective intervention for social improvements among older adults and gaming has been also found to reduce social anxiety and increase sociability [55]. A meta-analysis conducted in this review revealed a medium effect of exergaming intervention on the social functioning of older people. Exergaming interventions improved social relationships and reduced loneliness in three studies [35, 36, 40], while playing traditional games and board games did not [36, 40]. More research is needed about the effects of exergaming on social functioning measured by different scales, the ones focusing more on social participation, for example, the Social Engagement Scale. In the future, whether playing in a group is more effective in terms of social functioning than playing alone should also be investigated.
Kahlbaugh et al. [53] found that older people with a positive mood are more physically active and feeling less lonely is the greatest predictor of a positive mood. In the current review, playing Nintendo Wii Fit and Sports games increased the physical activity of older people living in long-term care. In all three studies where physical activity increased, exergames were played in groups [30, 36, 42]. In Carrasco et al. [56], playing Nintendo Wii Sports did not increase the physical activity of community-dwelling older people. Independently living older people are probably more active in their everyday life than long-term care residents, so exergaming intervention might be more effective on this less active population. Longitudinal research about the maintenance of physical activity after the intervention period would be important to study in the future. In all studies selected for this review, physical activity was measured by a self-reported questionnaire. None of the studies used an activity bracelet that would measure activity objectively.
None of the studies included in this review compared outcome results between gender. Therefore, there is no evidence on whether exergaming is more beneficial for other gender. In 9 of the 15 studies, majority of the participants were women, but there were no gender differences in the groups compared in the studies. Because women live longer than men, most long-term care facility residents are usually women, which explains the uneven gender distribution in the studies.
Strengths and limitations
The strength of this review is that it synthesizes the effects of digital gaming on the wide-ranging functional ability of older people. We did not limit the interventions to a specific game or game device. There are some limitations to this study. Interventions, comparator groups, and participants varied widely across the studies, so the real effect is challenging to assess. A random-effect model was used in the meta-analysis to correct these effects. Studies selected for this review had small sample sizes, and only three had 60 or over 60 participants, which might lower the statistical power of the studies. We did not restrict studies to randomized-controlled trials, and we also included quasi-experimental studies. This might have caused bias in this study. However, RCT studies and quasi-experimental studies were separated in the meta-analysis. Only a few of the included studies examined psychological and social functioning, and social functioning was mainly measured as part of the quality of life. In two meta-analyses of psychological functioning, there were only two studies in both analyses. Therefore, social and psychological functioning results should be interpreted with caution. We included studies published only in English; therefore, studies that would have met the inclusion criteria may have been left out of this review.
Conclusions
Digital gaming interventions implemented in the long-term care context for older people focus on exergaming, and Nintendo Wii and XBox 360 Kinect are the most common game devices. Playing digital exergames seems to be effective in promoting older people’s physical and social functioning and in increasing their physical activity in a long-term care environment. Social activity was not measured in any study. Exergames can also be recommended for older people with mild cognitive and physical limitations to promote physical functioning. The effects in terms of psychological functioning are not completely clear, but playing exergames has been able to have a positive effect on the reduction of depressive symptoms. There is a lack of studies that use other kinds of gaming systems, such as mobile games, in interventions for older people. Playing with smart devices and different applications needs further investigation in the future. Implementation of digital gaming activities requires the competence of nursing staff and rehabilitation professionals in digitalization.
References
United Nation (2020) World population ageing 2020 highlights. https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd-2020_world_population_ageing_highlights.pdf. Accessed 4 Jan 2023
Zimmermann J (2022) Individual characteristics associated with the utilization of nursing care in the very old population: a cross-sectional study. BMC Geriatr 22:763. https://doi.org/10.1186/s12877-022-03448-y
Lotvonen S, Kyngäs H, Bloigu R et al (2018) Self-reported and measured physical performance among older people after 3 and 12 months of relocation to senior-housing [in finnish]. Hoitotiede 30:27–40
Lotvonen S, Kyngäs H, Koistinen P et al (2018) Mental well-being of older people in Finland during the first year in senior housing and its association with physical performance. Int J Environ Res Public Health 15:1331. https://doi.org/10.3390/ijerph15071331
McAuley E, Konopack JF, Morris KS et al (2006) Physical activity and functional limitations in older women: influence of self-efficacy. J Gerontol B Psychol Sci Soc Sci 61:270–277. https://doi.org/10.1093/geronb/61.5.P270
Diegelmann M, Jansen C, Wahl H et al (2018) Does a physical activity program in the nursing home impact on depressive symptoms? A generalized linear mixed-model approach. Aging Ment Health 22:784–793. https://doi.org/10.1080/13607863.2017.1310804
Chou C-H, Whang C-L, Wu Y-T (2012) Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: a meta-analysis. Arch Phys Med Rehabil 93:237–244. https://doi.org/10.1016/j.apmr.2011.08.042
Jantunen H, Wasenius N, Salonen MK et al (2017) Objectively measured physical activity and physical performance in old age. Age Ageing 46:232–237. https://doi.org/10.1093/ageing/afw194
Arrieta H, Rezola-Pardo C, Zarrazquin I et al (2018) A multicomponent exercise program improves physical function in long-term nursing home residents: a randomized controlled trial. Exp Gerontol 103:94–100. https://doi.org/10.1016/j.exger.2018.01.008
Zar A, Ahmadi F, Hoseini SA et al (2022) An investigation into the health related quality of life (HRQoL) of older women living in nursing homes in Iran with particular reference to physical activity. Cities 131:103885. https://doi.org/10.1016/j.cities.2022.103885
Chen Y (2010) Perceived barriers to physical activity among older adults residing in long-term care institutions. J Clin Nurs 19:432–439. https://doi.org/10.1111/j.1365-2702.2009.02990.x
Baert V, Gorus E, Mets T et al (2011) Motivators and barriers for physical activity in the oldest old: a systematic review. Ageing Res Rev 10:464–474. https://doi.org/10.1016/j.arr.2011.04.001
Van Malderen L, Mets T, Gorus E (2012) Interventions to enhance the quality of life of older people in residential long-term care: a systematic review. Ageing Res Rev 12:141–150. https://doi.org/10.1016/j.arr.2012.03.007
Staiano AE, Calvert S (2011) Exergames for physical education courses: physical, social, and cognitive benefits. Child Dev Perspect 5:93–98. https://doi.org/10.1111/j.1750-8606.2011.00162.x
Choi SD, Guo L, Kang D et al (2017) Exergame technology and interactive interventions for elderly fall prevention: a systematic literature review. Appl Ergon 65:570–581. https://doi.org/10.1016/j.apergo.2016.10.013
Orsega-Smith EM, Kalksma PJ, Harris W et al (2021) Older adults and exergames Olympics: feasibility and fun. Act Adapt Aging 45:118–134. https://doi.org/10.1080/01924788.2020.1728044
Valenzuela T, Okubo Y, Woodbury A et al (2018) Adherence to technology-based exercise programs in older adults: a systematic review. J Geriatr Phys Ther 41:49–61. https://doi.org/10.1519/JPT.0000000000000095
Dobbins S, Hubbard E, Flentje A et al (2020) Play provides social connection for older adults with serious mental illness: A grounded theory analysis of a 10-week exergame intervention. Aging Ment Health 24:596–603. https://doi.org/10.1080/13607863.2018.1544218
Li J, Erdt M, Chen L et al (2018) The social effects of exergames on older adults: systematic review and metric analysis. J Med Internet Res 20:e10486. https://doi.org/10.2196/10486
Ren Y, Savadlou A, Park S et al (2023) The impact of loneliness and social isolation on the development of cognitive decline and Alzheimer’s Disease. Front Neuroendocrinol 69:101061. https://doi.org/10.1016/j.yfrne.2023.101061
Bonnechère B, Langley C, Sahakian BJ (2020) The use of commercial computerised cognitive games in older adults: a meta-analysis. Sci Rep 10:15276. https://doi.org/10.1038/s41598-020-72281-3
Taylor LM, Kerse N, Frakking T et al (2018) Active video games for improving physical performance measures in older people: a meta-analysis. J Geriatr Phys Ther 41:108–123. https://doi.org/10.1519/JPT.0000000000000078
Cacciata M, Stromberg A, Lee J et al (2019) Effect of exergaming on health-related quality of life in older adults: a systematic review. Int J Nurs Stud 93:30–40. https://doi.org/10.1016/j.ijnurstu.2019.01.010
Martinho D, Carneiro J, Corchado JM et al (2020) A systematic review of gamification techniques applied to elderly care. Artif Intell Rev 53:4863–4901. https://doi.org/10.1007/s10462-020-09809-6
Aromataris E, Munn Z (2020) JBI manual for evidence synthesis. JBI. https://doi.org/10.46658/JBIMES-20-01
Page MJ, McKenzie JE, Bossuyt PM et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Higgins JPT (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560. https://doi.org/10.1136/bmj.327.7414.557
Delbroek T, Vermeylen W, Spildooren J (2017) The effect of cognitive-motor dual task training with the biorescue force platform on cognition, balance and dual task performance in institutionalized older adults: a randomized controlled trial. J Phys Ther Sci 29:1137–1143. https://doi.org/10.1589/jpts.29.1137
Swinnen N, Vandenbulcke M, de Bruin ED et al (2021) The efficacy of exergaming in people with major neurocognitive disorder residing in long-term care facilities: a pilot randomized controlled trial. Alzheimers Res Ther 13:70. https://doi.org/10.1186/s13195-021-00806-7
Janssen S, Tange H, Arends R (2013) A preliminary study on the effectiveness of exergame Nintendo “Wii Fit Plus” on the balance of nursing home residents. Games Health J 2:89–95. https://doi.org/10.1089/g4h.2012.0074
Mugueta-Aguinaga I, Garcia-Zapirain B (2017) FRED: exergame to prevent dependence and functional deterioration associated with ageing a pilot three-week randomized controlled clinical trial. Int J Environ Health Res 14:1439. https://doi.org/10.3390/ijerph14121439
Cicek A, Ozdincler AR, Tarakci E (2020) Interactive video game-based approaches improve mobility and mood in older adults: a nonrandomized, controlled tri̇al. J Bodyw Mov Ther 24:252–259. https://doi.org/10.1016/j.jbmt.2020.01.005
Stanmore E, Mavroeidi A, de Jong L et al (2019) The effectiveness and cost-effectiveness of strength and balance Exergames to reduce falls risk for people aged 55 years and older in UK assisted living facilities: a multi-centre, cluster randomised controlled trial. BMC Med 17:49. https://doi.org/10.1186/s12916-019-1278-9
Fakhro MA, Hadchiti R, Awad B (2020) Effects of Nintendo Wii fit game training on balance among Lebanese older adults. Aging Clin Exp Res 32:2271–2278. https://doi.org/10.1007/s40520-019-01425-x
Chen ST, Huang YGL, Chiang IT (2012) Using somatosensory video games to promote quality of life for the elderly with disabilities. In: IEEE fourth international conference on digital game and intelligent toy enhanced learning, pp 258–262. https://doi.org/10.1109/DIGITEL.2012.68
Jung Y, Li K, Janissa N, Gladys W, Lee K (2009) Games for a better life: effects of playing Wii games on the well-being of seniors in a long-term care facility. In: IE 09: Proceedings of the sixth Australasian conference on interactive entertainment 5, pp 1–6. https://doi.org/10.1145/1746050.1746055
Yousefi Babadi S, Daneshmandi H (2021) Effects of virtual reality versus conventional balance training on balance of the elderly. Exp Gerontol 153:111498. https://doi.org/10.1016/j.exger.2021.111498
Padala KP, Padala PR, Malloy TR et al (2012) Wii-fit for improving gait and balance in an assisted living facility: a pilot study. J Aging Res 2012:597573. https://doi.org/10.1155/2012/597573
Soares AV, Borges NG, Hounsell M et al (2016) A serious game developed for physical rehabilitation of frail elderly. Neurophysiol Clin 46:281. https://doi.org/10.1016/j.neucli.2016.09.109
Rica RL, Shimojo GL, Gomes MC et al (2020) Effects of a Kinect-based physical training program on body composition, functional fitness and depression in institutionalized older adults. Geriatr Gerontol Int 20:195–200. https://doi.org/10.1111/ggi.13857
Ramnath U, Rauch L, Lambert EV et al (2021) Efficacy of interactive video gaming in older adults with memory complaints: a cluster-randomized exercise intervention. PLoS ONE 16:0252016. https://doi.org/10.1371/journal.pone.0252016
Keogh JWL, Power N, Wooller L et al (2014) Physical and psychosocial function in residential aged-care elders: effect of Nintendo Wii Sports games. J Aging Phys Act 22:235–244. https://doi.org/10.1123/japa.2012-0272
Zeng N, Pope Z, Lee JE et al (2017) A systematic review of active video games on rehabilitative outcomes among older patients. J Sport Health Sci 6:33–43. https://doi.org/10.1016/j.jshs.2016.12.002
Janhunen M, Karner V, Katajapuu N et al (2021) Effectiveness of exergame intervention on walking in older adults: a systematic review and meta-analysis of randomized controlled trials. Phys Ther 101:1. https://doi.org/10.1093/ptj/pzab152
Pacheco TBF, de Medeiros CSP, de Oliveira VHB et al (2020) Effectiveness of exergames for improving mobility and balance in older adults: A systematic review and meta-analysis. Syst Rev 9:163. https://doi.org/10.1186/s13643-020-01421-7
Zhao Y, Feng H, Wu X et al (2020) Effectiveness of exergaming in improving cognitive and physical function in people with mild cognitive impairment or dementia: systematic review. JMIR Serious Games. 8:e16841. https://doi.org/10.2196/16841
Zheng Guichen L, Xinxin W, Huiru Y et al (2020) Effect of exergames on physical outcomes in frail elderly: a systematic review. Aging Clin Exp Res 32:2187–2200. https://doi.org/10.1007/s40520-019-01344-x
Yen H, Chiu H (2021) Virtual reality exergames for improving older adults’ cognition and depression: a systematic review and meta-analysis of randomized control trials. J Am Med Dir Assoc 22:995–1002. https://doi.org/10.1016/j.jamda.2021.03.009
Eriksson S, Gard G (2011) Physical exercise and depression. Phys Ther Rev 16:261–268. https://doi.org/10.1179/1743288X11Y.0000000026
Bridle C, Spanjers K, Patel S et al (2012) Effect of exercise on depression severity in older people: systematic review and meta-analysis of randomised controlled trials. Br J Psychiatry 201:180–185. https://doi.org/10.1192/bjp.bp.111.095174
Holt-Lunstad J, Smith TB, Layton JB (2010) Social relationships and mortality risk: a meta-analytic review. PLoS Med 7:e1000316. https://doi.org/10.1371/journal.pmed.1000316
Hagan R, Manktelow R, Taylor BJ et al (2014) Reducing loneliness amongst older people: a systematic search and narrative review. Aging Ment Health 18:683–693. https://doi.org/10.1080/13607863.2013.875122
Kahlbaugh PE, Sperandio AJ, Carlson AL et al (2011) Effects of playing Wii on well-being in the elderly: physical activity, loneliness, and mood. Act Adapt Aging 35:331–344. https://doi.org/10.1080/01924788.2011.625218
Vázquez FL, Otero P, García-Casal JA et al (2018) Efficacy of video game-based interventions for active aging a systematic literature review and meta-analysis. PLoS ONE 13:e0208192. https://doi.org/10.1371/journal.pone.0208192
Xu X, Li J, Pham TP et al (2016) Improving psychosocial well-being of older adults through exergaming: the moderation effects of intergenerational communication and age cohorts. Games Health J 5:389. https://doi.org/10.1089/g4h.2016.0060
Carrasco M, Ortiz-Maqués N, Martínez-Rodríguez S (2020) Playing with Nintendo Wii sports: impact on physical activity, perceived health and cognitive functioning of a group of community-dwelling older adults. Act Adapt Aging 44:119–131. https://doi.org/10.1080/01924788.2019.1595261
Funding
Open Access funding provided by University of Oulu including Oulu University Hospital. This study was partly financially supported by Competitive State Research Financing.
Author information
Authors and Affiliations
Contributions
SK, SE, and HS contributed to study conception and design. Study selection and quality assessment were performed by SK, SE, HS, and SA. Data extraction was performed by SK. Data analysis was performed by SK and JM. The first draft of the manuscript was written by SK, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kukkohovi, S., Siira, H., Arolaakso, S. et al. The effectiveness of digital gaming on the functioning and activity of older people living in long-term care facilities: a systematic review and meta-analysis. Aging Clin Exp Res 35, 1595–1608 (2023). https://doi.org/10.1007/s40520-023-02459-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-023-02459-y