
Abstract
Purpose
The purpose of this article is to review the role of technical and nontechnical skills in routine and crisis situations. We discuss the role of different simulation modalities in addressing these skills and competencies to enhance patient safety.
Principal findings
Human and system errors are a recognized cause of significant morbidity and mortality. Technical skills encompass the medical and procedural knowledge required for patient care, while nontechnical skills are behaviour-based and include task management, situation awareness, teamwork, decision-making, and leadership. Both sets of skills are required to improve patient safety. Healthcare simulation can provide an opportunity to practice technical and nontechnical skills in a patient-safe environment. More specifically, these skills are most required in dynamic and crisis situations, which may best be practiced in a simulated patient setting.
Conclusion
Healthcare simulation is a valuable tool to improve patient safety. Simulation-based education can focus on the necessary technical and nontechnical skills to enhance patient safety. Simulation-based research can serve as a means to identify gaps in current practice, test different solutions, and show improved practice patterns by studying performance in a setting that does not compromise patient safety.
Résumé
Objectif
L’objectif de cet article est de passer en revue le rôle des compétences techniques et non techniques dans les situations courantes et les situations de crise. Nous discutons le rôle de différentes modalités de simulation pour aborder la question de ces compétences afin d’améliorer la sécurité du patient.
Constatations principales
Les erreurs humaines et de système sont une cause reconnue de morbidité et de mortalité significatives. Les compétences techniques englobent les connaissances médicales et procédurales nécessaires aux soins des patients, alors que les compétences non techniques sont fondées sur le comportement et comprennent la gestion de tâches, la prise de conscience de la situation, le travail d’équipe, la prise de décision et le leadership. Ces deux ensembles de compétences sont nécessaires à l’amélioration de la sécurité du patient. La simulation en soins de santé peut constituer une occasion d’exercer des compétences techniques et non techniques dans un environnement sécuritaire pour le patient. Plus spécifiquement, ces compétences sont nécessaires particulièrement dans les situations dynamiques ou de crise, et un environnement simulé est alors l’endroit idéal pour les exercer.
Conclusion
La simulation en soins de santé est un outil utile pour améliorer la sécurité du patient. La formation fondée sur la simulation peut être dirigée sur les compétences techniques et non techniques nécessaires afin d’améliorer la sécurité du patient. La recherche fondée sur la simulation peut constituer un moyen d’identifier les lacunes dans la pratique actuelle, de tester diverses solutions, et de montrer des schémas de pratique améliorés en étudiant la performance dans un cadre qui ne met pas en péril la sécurité du patient.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Errors create a case for improvement
The nature of human and system errors that lead to adverse outcomes has been investigated in complex systems, such as the commercial aviation industry and the nuclear power industry. These organizations are collectively known as “high-reliability organizations” (HROs), and detailed descriptions can be found in safety literature.1 High-reliability organizations are defined as high-risk error-intolerant systems that repeatedly carry out potentially dangerous procedures with minimal error. High-reliability organizations understand circumstances that are likely to lead to adverse events known as “error-producing conditions” (EPCs). After careful analysis of accidents and near-miss incidents, sets of these conditions have been established with the use of mathematical modelling of contributing factors.2,3
As business practices are increasingly applied to medicine, many have argued that healthcare could be viewed through the lens of an HRO. Technological advances in healthcare and evidence-based practices have improved care for our patients; however, now more than ever, we are aware of errors and the ways in which they compromise patient safety. Over a decade ago, The Institute of Medicine disclosed that error is a significant cause of death in the United States that accounts for 44,000 to potentially as many as 98,000 deaths annually.4,5 This magnitude makes errors more lethal than motor vehicle collisions, breast cancer, and AIDS.6 In Canada, approximately 7.5% of hospital admissions will result in an adverse event.7 What is more surprising than the frequency of these events is the realization that up to one-third of these events are highly preventable. Perhaps less surprising is the fact that most of these highly preventable events do not result from individual negligence but from the failure of systems and teams.
Five hallmarks of HROs that account for their less than expected number of accidents are: 1) preoccupation with failure; 2) reluctance to simplify interpretations; 3) sensitivity to operations; 4) commitment to resilience; and 5) deference to expertise. Together, these qualities are termed “mindfulness”.8
The most important EPCs common to all HROs are fatigue, high-risk low-frequency events, time pressures, normalization of deviancy, poor supervision, faulty perception of risk (injury severity), and task overload.2 In order to transform its “mindfulness”, the healthcare system must mitigate these EPCs. For example, the complexity of managing a trauma patient highlights the potential EPCs that can put patient safety at risk (Table 1).
Technical and nontechnical skills for patient safety
There is widespread recognition that all physicians and healthcare professionals require a broader set of competencies beyond medical expertise to improve the healthcare system. Medical knowledge and procedural ability map to a larger group of competencies that the simulation community commonly referred to as technical skills.9 These technical skills were the focus of most undergraduate and postgraduate curricula until the turn of the last century. Continuing medical education programs continue to focus nearly exclusively on technical skills. With the greater acknowledgement of system errors and their contribution to significant morbidity and mortality, there is a growing understanding that all healthcare professionals require another set of competencies. Task management, teamwork, leadership, situational awareness, and decision-making are some of the identified behaviours that may mitigate the risk of EPCs.10 In contrast to the traditional technical skills, the simulation community conventionally refers to these competencies as nontechnical skills (Table 2). Nontechnical skills have been identified as particularly important in emergency and crisis situations, which are dynamic, evolving, and require constant re-assessment.11
For physicians, in particular, regulatory bodies and professional colleges internationally have developed taxonomies of the required competencies to articulate and define further these broad technical and nontechnical skills. In Canada, we are most familiar with the CanMEDS competency framework, which defines competence over seven domains of equal importance but is recognized to centre on medical expert.12 The CanMEDS framework has been integrated into the lifelong learning model, which recognizes the need for ongoing continuous professional development. Thus, by definition, maintaining competence is dynamic and cannot be conferred for a lifetime based on static undergraduate or postgraduate examinations from a single point in time.13 In an attempt to extend the concept of competencies to teams, the Canadian Patient Safety Institute developed patient safety competencies that complement the non-medical expert competencies in CanMEDS and address safety beyond the level of the individual14 (Table 3).
Perhaps the most important consequence of identifying these nontechnical skills or non-medical expert competencies is the recognition that they are not inherent despite being based on behaviour.15 Any teaching of these competencies is accomplished informally in the clinical setting and probably attributed most to role modelling from mentors. Delivery of nontechnical skills solely by this process is potentially flawed as it is based on many assumptions. First, it assumes that faculty supervisors are experts in these competencies. Second, as mentioned earlier, many of these skills are required most during emergency or crisis situations, which are increasingly rare in modern day medicine. Finally, learning based entirely on role modelling may perpetuate negative learning where less than ideal behaviours can spread without assessment, feedback, and correction.16 Ideally, role modelling should be complemented with other education modalities.
Nontechnical skills must be formally taught, and in fact, probably more time is required to develop curriculum for these skills because they are more difficult to teach and assess than their technical skill counterparts.17 Without balanced curriculum design, the challenge in teaching nontechnical skills for patient safety can result in their overall marginalization. The biggest challenge to engage learners in these important competencies through conventional didactic instruction is the lack of context. Contextualizing these concepts can be beneficial for both faculty and learners as it can ease the instructional difficulties of teaching behaviours and facilitate sharing important mental models.18-20 By definition, most of these nontechnical skills are not practiced in isolation by any professional. An important aspect of translating mental models to a clinical context is incorporating an interprofessional faculty and audience. A mixed faculty and audience provide a variety of perspectives to appreciate the required communication and collaborative competencies. Other industries (i.e., military and aviation) have embraced interprofessional models for training.21 Team training in healthcare has included simulation to provide the appropriate context for interprofessionals to improve patient safety.19,22,23
Simulation modalities available for patient safety
Simulation can provide a forum for contextualized learning. As it relates to healthcare, simulation is defined as a technique rather than as a technology. It amplifies real patient experiences in a fully interactive manner.24 Simulation is an educational tool amongst many modalities that can improve patient safety directly by guiding clinical practice or indirectly through best education practice. While simulation is not the only tool in the arsenal of workplace or work-based contextualized lifelong learning, there is growing evidence that it is a powerful tool.
Over the last three decades, it has become more common to have trainees learn skills in medical history taking and physical examinations using standardized patients and to have them learn procedural skills using animal models.25 In the 21st century, advancements in engineering have ushered in a new era of simulator technology, including more complex partial-task trainers (i.e., models that replicate reality in a limited fashion to teach a specific delineated skill, such as central line placement or thoracentesis) and virtual reality simulators for surgical and procedural skills (i.e., hardware and software that provide haptic feedback for performing realistic laparoscopic cholecystectomy, bronchoscopy, colonoscopy, and echocardiography).
As mentioned previously, most consider that the strength of simulation to improve patient safety lies in modalities that address systems and team competence. For the anesthesiologist working in the operating room, patient safety is best addressed by mannequin-based simulation—the mode of simulation we pioneered and with which we are most familiar.26
The development of mannequins has advanced significantly over the last two decades, and software advances have allowed the most advanced mannequins to recognize injection of medications or therapeutic maneuvers, such as cardiac massage, and to respond in an appropriate physiologic manner. When preprogrammed responses are not available, mobile technology allows real-time physiologic manipulation; however, it would be a mistake to focus on these technological mannequins to improve safety alone. In fact, instead of precise replication, there is mounting evidence that only lower fidelity may be needed to approximate a simulator’s true anatomy and physiology.27-29 Patient safety educators dedicated to improving nontechnical skills focus their programs on improving the environmental fidelity of their scenarios.
Environmental fidelity refers to the relationship between the simulation learning environment and the setting in clinical practice.30 Improving the environmental fidelity means incorporating all the structural and mechanized elements that would be present in the management of similar scenarios in the clinical realm. As discussed, the most important aspect is assembling a similar interprofessional cohort that would manage patients in the clinical environment. Fidelity is enhanced when the interprofessional team is dressed as they would be for clinical activities. This can be particularly important for the anesthesiologist, as it forces the team to address communication barriers unique to our environment, such as role identification and the interpretation of non-verbal cues when offered behind masks and surgical gowns. The costs to re-create all of these important clinical elements in a simulation centre can be prohibitive. In-situ simulation in an actual clinical setting can mitigate these costs, with the only expenses being the simulator, human resources, and disposables. This approach also potentially addresses barriers in assembling interprofessional teams for an educational activity during working hours. Recent advances in wireless technology have facilitated operationalizing in situ simulation, and they are recognized as solutions to increasing fidelity in the absence of simulation centre resources.
When live interaction between different health professions is unavailable, current research is also preserving fidelity by practicing communication and collaboration in a virtual environment.31,32 From isolated settings, doctors, nurses, and other allied health professions can work together online in the management of Web-based patient scenarios.33 While fidelity may not be optimized as in a live environment, this interprofessional learning supports the importance of team interaction and may be particularly applicable to the geography of Canada.
Simulation-based education: how it works
The success of simulation as a learning modality can be summarized by four basic principles: pattern recognition, the interplay of emotions and learning, the effectiveness of debriefing, and the importance of deliberate practice.
First, pattern recognition has been defined as the probability and efficiency of retrieving an item from memory. Pattern recognition depends on the similarity of the conditions in which an item has been encoded to memory and the similarity of the conditions in which it needs to be retrieved.34 With simulation, a healthcare professional can be exposed not only to rarely encountered clinical scenarios but also to learning in an almost identical clinical context where the skills will be required.
Second, there is evidence that learning can be more constructive when emotions are engaged. With simulation, learners are often confronted with situations that spark curiosity, perplexity, and confusion that can enhance learning if managed well by faculty.35 Faculty development is required to manage the delicate balance of emotions and learning effectively through feedback from direct observations in a debriefing – a hallmark of simulation-based education.36
Simulation-based education is based on the experiential learning cycle where learners participate in a scenario or procedure and manage the entire task from the beginning to a predetermined end to the scenario.37 Following the scenario, a trained instructor provides feedback in a debriefing session, often with video playback, so learners can reflect on both the positive and negative aspects of their performance.38 The cycle is completed by allowing trainees the opportunity to compare their performances with their existing knowledge and also to participate in the same scenario or a similar scenario requiring the identical skills.39
Deliberate practice refers to a process that allows learners to focus on intensive practice of specific tasks in a controlled setting while receiving coaching and formative assessment through timely and thoughtful feedback from an expert supervisor.40 A main feature of deliberate practice is that it occurs over a long time period and requires many hours to advance from novice to expert. Expertise in medicine, as in athletics, chess, and music, is closely related to the amount of time devoted to deliberate practice.41 Simulation is ideal for deliberate practice because it offers standardized conditions and the ability to repeat the same tasks frequently without compromising patient safety.
Simulation-based education: maintaining competency
Recognizing the importance of deliberate practice is closely associated with acknowledging that even mastered skills will most likely decay if not exercised regularly.42 Almost every anesthesiologist will experience the stress of managing a difficult airway and, more specifically, the “can’t intubate, can’t ventilate” situation; however, with an incidence of approximately one in 10,000, both the technical and nontechnical skills required to manage these crises have not been rehearsed, practiced, or experienced in months or even years.43 Decay and attrition of skills is inevitable and demonstrable.44 Ultimately, it is equally important to develop lifelong learning strategies to manage crises as it is to manage knowledge translation and retention more effectively.45 Simulation may be a powerful enabler in the development of these strategies.
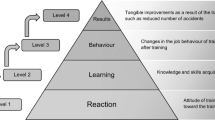
Furthermore, equally important as the development of education programs is the increasing need for physicians, as a self-regulated profession, to demonstrate accountability to the government and the public by creating assessment strategies that ensure they maintain their competence. Taxonomies of assessment, such as Miller’s pyramid, are useful to enable us to identify different levels of performance that may be assessed with different tools.46 With multiple-choice questions and oral examinations, we can assess the “knows” level of factual information. When designed to be rich in a clinical context, we can use the same tools to probe the integration of that knowledge into clinical judgement and decision-making, the “knows how” level of assessment.47 It has been suggested that simulation has advantages over other exam modalities in the domain of crisis management because it can assess what trainees would actually do rather than what they write or say, the “shows how” level of performance.48 More importantly, with simulation, we can potentially assess the competency of learners in a way that reflects actual clinical practice more closely than other assessment methods. By better replicating clinical practice, simulation allows for simultaneous assessment of multiple competencies, both technical and nontechnical. The “does” level of assessment can be performed only in the workplace where logistical and patient safety issues present challenges in this complex and dynamic setting. Thus, simulation may offer the best alternative to workplace assessment by providing a medium for work-based assessment.
Simulation research to demonstrate improved patient safety
Simulation has a great capacity to inform the patient safety movement and guide best practices for patient safety. Simulation can be used as an “object” of research, validating its efficacy as an educational tool, or it can be used as a “means” of research to study clinician performance in a patient-safe environment that is similar to the clinical setting.
The “gold standard” in validating simulation for patient safety is translational science. Traditionally, translational science has referred to biomedical research that advances or accelerates the application of results from the laboratory to patient care.49 Simulation research meets the criteria of translational science when it can demonstrate that the learning in a simulation laboratory impacts actual patient care. The T1 realm of simulation research would exhibit performance improvements in the simulation environment, while the T2 realm would demonstrate that the learning in the simulation laboratory translates directly to improved performance on patients. The T3 realm of research would improve the overall health of patients and society.50 Given the breadth of simulation literature and the importance of translational science on patient safety, this discussion focuses on the T2 and T3 realms of simulation research.
Procedural skills simulators have garnered the most attention in the patient safety movement, and T2 research has demonstrated that skills learned on simulators reduce the risk of errors by trainees when compared with traditional apprenticeship models of medical education. For example, learning laparoscopic cholecystectomy surgery on virtual reality simulators has led to a demonstrable reduction in predefined errors on patients in the operating room when compared with conventional instruction.51,52 Even more powerful is T3 evidence that individual procedural competence can be mastered through using simulators to gain expertise in complications of sepsis caused by central venous catheter insertion and brachial plexus injuries due to shoulder dystocia.53-55 Further research will determine whether simulated performance of the skills or familiarity with a procedural process is most responsible for the reduction in errors and, consequently, the improvements in patient safety.56 Ultimately, re-creating the clinical context and practicing processes may be more essential than incorporating a particular procedural simulator technology into a curriculum.57,58
Validating mannequin-based simulation with T2 and T3 research is far more challenging. As discussed, mannequins are used predominantly to teach the management of clinical crises. Crises are clinical events that occur rarely but are “high-stakes” situations associated with significant morbidity and mortality. Since these situations are rare and unpredictable, it is difficult to measure the effectiveness of simulation education in the clinical context. Furthermore, there are ethical concerns involved in allowing trainees to manage a patient crisis fully without intervention from a senior clinician. As such, there is a paucity of prospective T2 and T3 research evaluating the impact of mannequin-based simulation on patient safety.
In a retrospective case control study, management of patients using the Advanced Cardiac Life Support (ACLS) techniques was examined and a comparison was made between the results of residents who had received training in a simulator and the results of those who had not.59 Results showed that residents who had learned on a simulator were more likely to adhere to the ACLS guidelines than those who had learned by more traditional methods. In a recent prospective randomized study, the effects of using simulation to train residents to wean patients from cardiopulmonary bypass were compared with the effects of using a traditional interactive seminar. This study showed that the residents trained with simulation were more successful in executing both the technical and nontechnical skills required to wean patients from cardiopulmonary bypass, and their skills were better retained compared with the residents trained in the traditional manner.60
By providing a similar mock complex clinical environment, simulation can provide a “means” to study and dissect the management of crises and procedures critically.44 By deconstructing our current practices, we may identify gaps and deficiencies that need to be addressed. Furthermore, simulation can provide an environment free from patient harm to study the introduction of new equipment and to learn strategies for effective and safe practice. Simulation can provide a platform and environment that better controls for confounding variables for stronger study designs in this area of research.
Ultimately, researchers will strive to examine the effects of simulation on patient morbidity and mortality, but the logistics and ethics of measuring outcomes prospectively have proven challenging for rare and unpredictable emergency situations. Nevertheless, Gaba has stated, “No industry in which human lives depend on the skilled performance of responsible operators has waited for unequivocal proof of the benefits of simulation [or crisis resource management] before embracing it.”61
Conclusion
Patient safety is the keystone of good patient care. In order to keep patients safe, healthcare professionals not only need safety competencies, they also need an understanding of the context in which errors occur. Error-producing conditions describe the context and environment where gaps in practice can lead to poor outcomes. Simulation is a powerful tool that can contextualize learning, assessment, and research of competencies and ultimately improve patient safety.
Key points
-
High Reliability Organizations (HROs) are preoccupied with potential failure; as a result, they have developed methods for effective management of unexpected situations in high-risk environments. Healthcare can be viewed through the lens of an HRO to address patient safety.
-
Technical skills (medical knowledge and procedural ability) and nontechnical skills are both required to mitigate Error Producing Conditions (EPCs).
-
Nontechnical skills include task management, teamwork, situation awareness, decision-making, and leadership. Nontechnical skills need to be taught.
-
Simulation-based education with interprofessional teams provides a context for learning nontechnical skills and facilitates sharing mental models. Environment fidelity is important as a context for learning.
-
Translational research is emerging to validate simulation-based education for patient safety.
References
Stahl KD, Brien SB. Reducing patient errors in trauma care. In: Cohn SM (Ed.). Acute Care Surgery and Trauma - Evidenced-Based Practice. Informa UK Ltd; 2009: 268-77.
Williams JC. A data-based method for assessing and reducing human error to improve operational performance. Monterey, CA, USA: IEEE fourth conference on human factors and power plants; 1988. p. 436-50.
Hendy KC. A Tool for Human Factors Accident Investigation, Classification and Risk Management. Defense R&D Canada – Toronto. Technical Report - DRDC Toronto TR 2002-057: 2003. Available from URL: http://i3pod.com/wp-content/uploads/2011/04/A-tool-for-human-factors-accident-invest-classification-risk-management-K-C-Hendy.pdf (accessed September 2012).
Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med 1991; 324: 377-84.
Thomas EJ, Studdert DM, Newhouse JP, et al. Costs of medical injuries in Utah and Colorado. Inquiry 1999; 36: 255-64.
Martin JA, Smith BL, Mathews TJ, Ventura SJ; Divisio of Vital Statistics. Centers for Disease Control and Prevention. (National Center for Health Statistics). Births and Deaths: Preliminary Data for 1998. National Vital Statistics Reports 1999. Available from URL: http://www.cdc.gov/nchs/data/nvsr/nvsr47/nvs47_25.pdf (accessed September 2012).
Baker GR, Norton PG, Flintoft V, et al. The Canadian Adverse Events Study: the incidence of adverse events among hospital patients in Canada. CMAJ 2004; 170: 1678-86.
Weick KE, Sutcliffe KM. Managing the Unexpected. San Francisco, CA: Jossey-Bass; 2001. p. 10.
Gaba DM, Howard SK, Flanagan B, Smith BE, Fish KJ, Botney R. Assessment of clinical performance during simulated crises using both technical and behavioral ratings. Anesthesiology 1998; 89: 8-18.
Flin R, Yule S, Paterson-Brown S, Maran N, Rowley D, Youngson G. Teaching surgeons about non-technical skills. Surgeon 2007; 5: 86-9.
Fletcher G, Flin R, McGeorge P, Glavin R, Maran N, Patey R. Rating non-technical skills: developing a behavioural marker system for use in anaesthesia. Cognition, Technology & Work 2004; 6: 165-71.
Frank JR, Danoff D. The CanMEDS initiative: implementing an outcomes-based framework of physician competencies. Med Teach 2007; 29: 642-7.
Naik VN, Wong AK, Hamstra SJ. Review article: Leading the future: guiding two predominant paradigm shifts in medical education through scholarship. Can J Anesth 2012; 59: 213-23.
Frank JR, Brien S, The Safety Competencies Steering Committee. The Safety Competencies: Enhancing Patient Safety Across the Health Professions. Ottawa, ON: Canadian Patient Safety Institute; 2008 .
Yee B, Naik VN, Joo HS, et al. Nontechnical skills in anesthesia crisis management with repeated exposure to simulation-based education. Anesthesiology 2005; 103: 241-8.
O’Sullivan H, van Mook W, Fewtrell R, Wass V. Integrating professionalism into the curriculum: AMEE Guide No. 61. Med Teach 2012; 34: e64-77.
Issenberg SB, McGaghie WC, Hart IR, et al. Simulation technology for health care professional skills training and assessment. JAMA 1999; 282: 861-6.
Kassab E, Kyaw Tun J, Kneebone RL. A novel approach to contextualized surgical simulation training. Simul Healthc 2012; 7: 155-61.
Paige JT. Surgical team training: promoting high reliability with nontechnical skills. Surg Clin North Am 2010; 90: 569-81.
Park CS. Simulation and quality improvement in anesthesiology. Anesthesiol Clin 2011; 29: 13-28.
Salas E, DiazGranados D, Weaver SJ, King H. Does team training work? Principles for health care. Acad Emerg Med 2008; 15: 1002-9.
Wilson KA, Burke CS, Priest HA, Salas E. Promoting health care safety through training high reliability teams. Qual Saf Health Care 2005; 14: 303-9.
Park CS, Rochlen LR, Yaghmour E, et al. Acquisition of critical intraoperative event management skills in novice anesthesiology residents by using high-fidelity simulation-based training. Anesthesiology 2010; 112: 202-11.
Gaba DM. The future vision of simulation in health care. Qual Saf Health Care 2004; 13(Suppl 1): i2-10.
Rosen KR. The history of medical simulation. J Crit Care 2008; 23: 157-66.
Denson JS, Abrahamson S. A computer-controlled patient simulator. JAMA 1969; 208: 504-8.
Brydges R, Carnahan H, Rose D, Rose L, Dubrowski A. Coordinating progressive levels of simulation fidelity to maximize educational benefit. Acad Med 2010; 85: 806-12.
Matsumoto ED, Hamstra SJ, Radomski SB, Cusimano MD. The effect of bench model fidelity on endourological skills: a randomized controlled study. J Urol 2002; 167: 1243-7.
Grober ED, Hamstra SJ, Wanzel KR, et al. The educational impact of bench model fidelity on the acquisition of technical skill: the use of clinically relevant outcome measures. Ann Surg 2004; 240: 374-81.
Halamek LP. The simulated delivery-room environment as the future modality for acquiring and maintaining skills in fetal and neonatal resuscitation. Semin Fetal Neonatal Med 2008; 13: 448-53.
Cook DA, Erwin PJ, Triola MM. Computerized virtual patients in health professions education: a systematic review and meta-analysis. Acad Med 2010; 85: 1589-602.
Sijstermans R, Jaspers MW, Bloemendaal PM, Schoonderwaldt EM. Training inter-physician communication using the Dynamic Patient Simulator. Int J Med Inform 2007; 76: 336-43.
Dye J, Gillon L, Sales R. Benefits and challenges of interprofessional collaboration in the development of a virtual learning environment. J Interprof Care 2009; 23: 95-7.
Norman GR, Brooks LR, Cunnington JP, Shali V, Marriott M, Regehr G. Expert-novice differences in the use of history and visual information from patients. Acad Med 1996; 71(10 Suppl): S62-4.
Russell JA. A circumplex model of affect. J Personality and Social Psychology 1980; 39: 1161-78.
Issenberg SB, Mcgaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach 2005; 27: 10-28.
Fanning RM, Gaba DM. The role of debriefing in simulation-based learning. Simul Healthc 2007; 2: 115-25.
Savoldelli GL, Naik VN, Park J, Joo HS, Chow R, Hamstra SJ. Value of debriefing during simulated crisis management: oral versus video-assisted oral feedback. Anesthesiology 2006; 105: 279-85.
Rudolph JW, Simon R, Rivard P, Dufresne RL, Raemer DB. Debriefing with good judgment: combining rigorous feedback with genuine inquiry. Anesthesiol Clin 2007; 25: 361-76.
Leblanc VR. Review article: simulation in anesthesia: state of the science and looking forward. Can J Anesth 2012; 59: 193-202.
Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med 2004; 79(10 Suppl): S70-81.
McGaghie WC, Siddall VJ, Mazmanian PE, Myers J, American College of Chest Physicians Health and Science Policy Committee. Lessons for continuing medical education from simulation research in undergraduate and graduate medical education: effectiveness of continuing medical education: American College of Chest Physicians Evidence-Based Educational Guidelines. Chest 2009; 135(3 Suppl): 62S-8S.
Heard AM, Green RJ, Eakins P. The formulation and introduction of a ‘can’t intubate, can’t ventilate’ algorithm into clinical practice. Anaesthesia 2009; 64: 601-8.
Wong DT, Lai K, Chung FF, Ho RY. Cannot intubate-cannot ventilate and difficult intubation strategies: results of a Canadian national survey. Anesth Analg 2005; 100: 1439-46.
Boet S, Borges BC, Naik VN, et al. Complex procedural skills are retained for a minimum of 1 yr after a single high-fidelity simulation training session. Br J Anaesth 2011; 107: 533-9.
Miller G. The assessment of clinical skills/competence/performance. Acad Med 1990; 65: S63.
Epstein R. Assessment in medical education. N Engl J Med 2007; 356: 387.
Savoldelli GL, Naik VN, Joo HS, et al. Evaluation of patient simulator performance as an adjunct to the oral examination for senior anesthesia residents. Anesthesiology 2006; 104: 475-81.
Dougherty D, Conway PH. The “3T’s” road map to transform US health care. JAMA 2008; 299: 2319-21.
McGaghie WC, Draycott TJ, Dunn WF, Lopez CM, Stefanidis D. Evaluating the impact of simulation on translational patient outcomes. Simulation in Healthcare 2011; 6: s42-7.
Grantcharov TP, Kristiansen VB, Bendix J, Bardram L, Rosenberg J, Funch-Jensen P. Randomized clinical trial of virtual reality simulation for laparoscopic skills training. Br J Surg 2004; 91: 146-50.
Ahlberg G, Enochsson L, Gallagher AG, et al. Proficiency-based virtual reality training significantly reduces the error rate for residents during their first 10 laparoscopic cholecystectomies. Am J Surg 2007; 193: 797-804.
Barsuk JH, McGaghie WC, Cohen ER, O’Leary KJ, Wayne DB. Simulation-based mastery learning reduces complications during central venous catheter insertion in a medical intensive care unit. Crit Care Med 2009; 37: 2697-701.
Barsuk JH, McGaghie WC, Cohen ER, Balachandran JS, Wayne DB. Use of simulation based mastery learning to improve the quality of central venous catheter placement in a medical intensive care unit. J Hosp Med 2009; 4: 397-403.
Draycott TJ, Crofts JF, Ash JP, et al. Improving neonatal outcome through practical shoulder dystocia training. Obstet Gynecol 2008; 112: 14-20.
Ma IW, Brindle ME, Ronksley PE, Lorenzetti DL, Sauve RS, Ghali WA. Use of simulation-based education to improve outcomes of central venous catheterization: a systematic review and meta-analysis. Acad Med 2011; 86: 1137-47.
Dieckmann P, Gaba D, Rall M. Deepening the theoretical foundations of patient simulation as social practice. Simulation in Healthcare 2007; 2: 183-93.
Dieckmann P, Manser T, Wehner T, Rall M. Reality and fiction cues in medical patient simulation: An interview study with anesthesiologists. Journal of Cognitive Engineering and Decision Making 2007; 1: 148-68.
Wayne DB, Didwania A, Feinglass J, Fudala MJ, Barsuk JH, McGaghie WC. Simulation-based education improves quality of care during cardiac arrest team responses at an academic teaching hospital: a case-control study. Chest 2008; 133: 56-61.
Bruppacher HR, Alam SK, LeBlanc VR, et al. Simulation-based training improves physicians’ performance in patient care in high-stakes clinical setting of cardiac surgery. Anesthesiology 2010; 112: 985-92.
Gaba DM. Improving anesthesiologists’ performance by simulating reality. Anesthesiology 1992; 76: 491-4.
Financial support
None.
Conflict of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Naik, V.N., Brien, S.E. Review article: Simulation: a means to address and improve patient safety. Can J Anesth/J Can Anesth 60, 192–200 (2013). https://doi.org/10.1007/s12630-012-9860-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-012-9860-z