
Summary
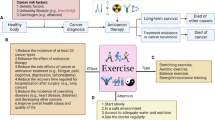
The level of physical activity represents a strong predictor of the cardiovascular long-term prognosis both in primary and secondary prevention.
The analysis of epidemiologic studies reveals a logarithmic regression between the relative cardiac risk RR and the weekly caloric expenditure (“physical activity”) E in kcal: RR = 1,23 – 0,06 ln E (kcal) (r = 0,58; p < 0,0001). The relation between the relative risk and the exercise capacity (“physical fitness”) seems to show an exercise threshold and tend to plateau (Sshape curve). A relative risk reduction of 20 – 25 % can be achieved both by an additional weekly energy expenditure of 1000 – 1500 kcal and by an increase of exercise capacity.
Based on physical and physiologic considerations, the mechanical and metabolic generated power P of muscles Pmech (kcal/min) = 0,01433 work load (W) and Pmet (kcal/min) = 0,06 work load (W), respectively, as well as the efficiency n = Pmech/Pmet = 0,24 can be calculated.
The total energy expenditure E (kcal) during ergometer training, f. i., can be estimated from the intensity or work load, expressed as watts and the duration of the training session t (min) by: E (kcal) = 0,06 work load (W) t (min).
Giving the energy expenditure in metabolic equivalents METs (1 MET = 3,5 ml 02/min/kg), the following equations can be used: work load (W) = 0,28 (METs – 1) body weight (kg) and METs = 1 + work load (W)/0,28 body weight (kg), respectively. The caloric expenditure amounts E (kcal) = 0,02 (METs – 1) t (min) body weight (kg).
Applying these considerations and tables of energy requirements for various activities, the energy expenditure of a moderate aerobic training program can be calculated.
To increase the work capacity, the prescribed exercise intensity should be below the individual anaerobic threshold (IANS) to avoid a marked sympathetic activation, especially in coronary patients. Typically, exercise intensity is expressed as a percentage of the maximal capacity in absolute terms (i. e. watts) or relative to the maximal heart rate, heart rate reserve, maximal oxygen uptake, or perceived exertion.
By analyzing the blood lactate curves of coronary patients with normal or slight reduced left ventricular ejection fraction we found, that the IANS was reached at 71 % of Wmax, and 80 % of the IANS (“safety margin”) were achieved at 57 % of Wmax. This corresponds to an exercise intensity ranging from 50 – 75 % of Wmax (values from the literature are 50 – 80 %). Between %Wmax at 80 % of the IANS and Wmax in absolute terms a linear regression can be calculated (r = 0.94; p < 0.005). From this a safe initial exercise intensity can be determined for coronary patients with approximately normal left ventricular function.
Zusammenfassung
Der Grad körperlicher Aktivität („physical activity“) stellt einen starken Prädiktor für die kardiovaskuläre Langzeitprognose sowohl in der Primär- als auch Sekundärprävention dar.
Eine Analyse epidemiologischer Studien ergab eine logarithmische Regression zwischen relativem kardialen Risiko (RR) und dem wöchentlichen Energieverbrauch E in kcal: RR = 1,23 – 0,06 ln E (kcal) (r = 0,58, p < 0,0001). Die Beziehung zwischen RR und der körperlichen Leistungsfähigkeit („physical fitness“) zeigt einen S-förmigen Verlauf mit einem Schwellenwert und Plateau. Eine relative Risikoreduktion von 20 – 25 % ist sowohl durch einen Mehrverbrauch von 1000 – 1500 Kilokalorienals auch durch eine Steigerung der Leistungsfähigkeitzu erreichen.
An Hand physikalischer und physiologischer Grundlagen werden die mechanisch und metabolisch erbrachte Leistung P (Power) der arbeitenden Muskulatur Pmech = 0,01433 Belastung (W) bzw. Pmet = 0,06 Belastung (W) sowie der Wirkungsgrad n = Pmech/Pmet = 0,24 berechnet. Der Energieverbrauch E, z. B. bei Ergometertraining, errechnet sich aus der Belastung in Watt (W) im Zeitabschnitt t (min) nach: E (kcal) = 0,06 Belastung (W) t (min). Wird der Energieverbrauch in metabolischen Äquivalenten METs (1 MET = 3,5 ml 02/min/kg) angegeben, kann unter Berücksichtigung des Körpergewichtes (kg) umgerechnet werden: Belastung P (W) = 0,28 (METs – 1) Körpergewicht (kg) bzw. METs = 1 + Belastung P (W)/0,28 Körpergewicht (kg). Der Energieverbrauch E in kcal beträgt wiederum: E (kcal) = 0,02 (METs – 1) t (min) Körpergewicht (kg).
Unter Anwendung dieser Beziehungen und entsprechender Tabellenwerke kann der Energieverbrauch bei einem “moderaten” aeroben Trainingsprogramm berechnet werden; z. B. ergeben bei einem Körpergewicht von 80 kg tägliches Ergometertraining mit 75 W, zügiges Gehen mit 6 km/h oder Radfahren mit 15 km/h über jeweils 30 Minuten einen wöchentlichen Mehrverbrauch von ca. 1075 kcal.
Bei der Verordnung der Trainingsintensität zur Steigerung der Leistungsfähigkeit wird ein dynamisches Ausdauertraining unterhalb der individuellen anaeroben Schwelle (IANS) also optimal und sicher angesehen, um eine ausgeprägte sympathiko- adrenerge Aktivierung mit ischämie-triggernden, vasokonstriktorischen und arrhythmogenen Effekten zu vermeiden. Es bestehen zahlreiche Empfehlungen, die sich auf die im Belastungstest erreichte maximale Herzfrequenz, die Leistungsfähigkeit, Sauerstoffaufnahme, Herzfrequenzreserve oder den subjektiven Anstrengungsgrad beziehen.
Wir fanden bei der Analyse der Lactat-Leistungskurven von Patienten mit koronarer Herzkrankheit und niedrig normaler Ejektionsfraktion, dass die IANS im Mittel bei 71 % von Wmax und 80 % der IANS („safety margin“) bei 57 % von Wmax erreicht werden. Unter Berücksichtigung der Standardabweichung entspricht dies in unserem Kollektiv einem Trainingsbereich von 50 – 75 % von Wmax. Zwischen %Wmax bei 80 % der IANS und der absoluten Belastungskapazität Wmax besteht eine lineare Beziehung (r = 0,94; p < 0,005). Für dieses Kollektiv lässt sich somit eine sichere initiale Trainingsintensität ermitteln.
Similar content being viewed by others


Literatur
Ades PHA (2001) Cardiac Rehabilitation and secondary prevention of coronary heart disease. N Engl J Med 345: 892–902
Balady GJ, Williams Mark A, Ades PHA, Bittner V, Comoss P, Foody JM, Franklin B, Sanderson B, Southard D (2007) Core components of cardiac Rehabilitation/Secondary prevention programs: 2007 Update. Circulation 115: 2675–2682
Blair SN, Kampert JB, Kohl HW, Barlow CE, Macera CA, Paffenberger RS, Gibbons LW (1996) Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and All-Cause Mortality in Men and Women. JAMA 276: 205–210
Blair SN, Kohl HW, Barlow CE, Macera CA, Paffenberger RS, Gibbons LW (1995) Changes in Physical Fitness and All-Cause Mortality. JAMA 273: 1093–1098
Kokkinos P, Myers J (2010) Exercise and Physical Acvtivity. Circulation 122: 1637–1648
Lavie CJ, Thomas RJ, Squires RW, Allison TG, Milani RV (2009) Exercise Training and Cardiac Rehabilitation in Primary and Secondary Prevention of Coronary Heart Disease. Mayo Clin Proc 84(4): 373–383
Shiroma EJ, Lee IM (2010) Physical Activity and Cardiovascular Health. Circulation 122: 743–752
Gielen S, Schuler G, Adams V (2010) Cardiovascular Effects of Exercise Training. Circulation 122: 1221–1238
De Backer G et al (2003) European guidelines on cardiovascular disease prevention in clinical practice. Eur J Cardiovasc Prevention and Rehabilitation 10: S1–S78
Froelicher, VRF, Myers, J (eds) (2006) Exercise and the Heart (5th ed). Saunders & Elsevier, Philadelphia
Gianuzzi P, Mezzani A, Saner H, Björnstad H, Fioretti P, Mendes M, Cohen-Solal A, Dugmore L, Hambrecht R, Hellemans I, Mc Gee H, Perk J, Vanhees L, Feress G (2003) Physical activity for primary and secondary prevention. Position Paper of the working group on cardiac rehabilitation. Eur J Cardiovasc Prevention and Rehabilitation 10: 319–327
JoliffeJA. Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S (2001) Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev 1: CD001800
Hammill BG, Curtis LH, Schulman KA, Whellan DJ (2010) Relationship Between Cardiac Rehabilitation and Long-Term Risks of Death and Myocardial Infarction Among Elderly Medicare Beneficiaries. Circulation 121: 63–70
Lloyd-Jones Donald M et al (2010) Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction. Circulation 121: 586–613
Niebauer J, Cooke JP (1996) Cardiovascular Effects of Exercise: Role of endothelial shear stress. J Am Coll Cardiol 28: 1652–1660
Niebauer J, Hambrecht R, Felich T, Hauer K, Marburger CH, Kälberer B, Weiss C, von Hodenberg E, Schlierf G, Schuler G, Zimmermann R, Kübler W. (1997) Attenuated progression of coronary artery disease after 6 years of multifactorial risk intervention. Circulation 96: 2534–2541
Niebauer J, Schuler G (2001) Antiatherogene Wirkungsmechanismen des körperlichen Trainings bei Patienten mit koronarer Herzkrankheit. Z Kardiol 90: 799–806
Williams PT (2010) Usefulness of Cardiorespiratory Fitness to Predict Coronary Heart Disease Risk Independent of Physical Activity. Am J Cardiol 106: 210–215
Kokkinos P, Myers J, Faselis C, Panagiotakos DB, Doumas M, Pittaras A, Manolis A, Kokkinos JP, Karasik P, Greenberg M, Papademetriou V, Fletcher R (2010) Exercise Capacity and Mortality in Older Men. Circulation 122: 790–797
Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE (2002) Exercise Capacity and mortality among men referred for exercise testing. N Engl J Med 346: 793–801
Myers J, Kaykha A, George S, Abella J, Zaheer N, Lear S, Yamazaki T, Froelicher V (2004) Fitness versus physical activity patterns in predicting mortality in men. Am J Med 117: 912–918
Dutcher JR, Kahn J, Grines C, Franklin B (2007) Comparison of left ventricular ejection fraction and exercise capacity as predictors of two- and five-year mortality following acute myocardial infarction. Am J Cardiol 99: 436–441
Pashkow, FJ, Dafoe, WA (eds) (1999) Clinical Cardiac Rehabilitation: A Cardiologist’s Guide (2nd ed). Williams & Williams, Baltimore
Redberg Rita F et al (2009) ACCF/AHA 2009 Performance Measures for Primary Prevention of Cardiovascular Disease in Adults. Circulation 120: 1296–1336
Sandvik L, Erikssen J, Thaulow E, Erikksen G, Mundal R, Rodahl K (1993) Physical fitness as a predictor of mortality among healthy, middleaged Norwegian men. N Engl J Med 328: 533–537
Mertens DJ, Kavanagh T, Shepard RJ (1994) A simple formula for the estimation of maximal oxygen intake during cycle ergometry. Eur Heart J 15: 1247–1251
Tegtbur U, Meyer H, Machold H, Busse MW (2002) Belastungsdiagnostische Kenngrößen und Katecholamine bei Koronarpatienten. Z Kardiol 91: 927–936
Heitkamp HC, Hipp A (2001) Lactat in der kardialen Rehabilitation. Herz 26: 447–453
Borg G. Borg’s Perceived exertion and pain scales. 1998, Human Kinetics
Bjarnason-Wehrens B, Schulz O, Gielen St, Halle M, Dürsch M, Hambrecht R, Lowis H, Kindermann W, Schulze R, Rauch B (2009) Leitlinie körperliche Aktivität zur Sekundärprävention und Therapie kardiovaskulärer Erkrankungen. Clin Res Cardiol Suppl 4: 1–44
Wolf R (2008) Laktat-Leistungsdiagnostik bei koronarer Herzkrankheit. Österr. J Sport Med 38: 32
Ziegler M, Reer, Braumann KM. Trainingssteuerung in der Bewegungstherapie. In: Halle M (Hrsg.). Sporttherapie in der Medizin. Schattauer GmbH, Stuttgart/New York, 2008: 27–34
Author information
Authors and Affiliations
Corresponding author
Additional information
Eingegangen am 4. April 2011, angenommen am 20. Oktober 2011
Exercise as cardiovascular therapy – how much is good and safe?
Rights and permissions
About this article
Cite this article
Wolf, R., Baumbach, C., Habel, F. et al. Körperliche Aktivität als kardiovaskuläre Therapie Wie viel ist gut und sicher?. Sportmed Präventivmed 41, 10–14 (2011). https://doi.org/10.1007/s12534-011-0209-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12534-011-0209-0
Keywords
- physical activity
- fitness level
- cardiovascular protection
- energy expenditure
- aerobic training
- anaerobic threshold
- exercise intensity