
Abstract
Opioid use disorder (OUD), a leading cause of morbidity and mortality in the USA, can be effectively treated with buprenorphine. However, the same pharmacologic properties (e.g., high affinity, partial agonism, long half-life) that make it ideal as a treatment for OUD often cause concern among clinicians that buprenorphine will prevent effective management of acute pain with full agonist opioid analgesics. Because of this concern, many patients are asked to stop buprenorphine preoperatively or at the onset of acute pain, placing them at high risk for both relapse and a difficult transition back to buprenorphine after acute pain has resolved. The purpose of this review is to summarize the existing literature for acute pain and perioperative management in patients treated with buprenorphine for OUD and to provide practical management recommendations for generalist practitioners based on evidence and clinical experience. In short, evidence suggests that sufficient analgesia can be achieved with maintenance of buprenorphine and use of both opioid and non-opioid analgesic options for breakthrough pain. We recommend that clinicians (1) continue buprenorphine in the perioperative or acute pain period for patients with OUD; (2) use a multi-modal analgesic approach; (3) pay attention to care coordination and discharge planning when making an analgesic plan for patients with OUD treated with buprenorphine; and (4) use an individualized approach founded upon shared decision-making. Clinical examples involving mild and severe pain are discussed to highlight important management principles.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Opioid use disorder (OUD) is a chronic disease affecting 2.1 million Americans,1 and opioid-related overdose is one of the leading causes of preventable mortality for Americans.2 Many patients with OUD also suffer from pain. Buprenorphine, a semi-synthetic opioid, was first developed in the 1970s as an analgesic with parenteral and sublingual formulations.3 It was subsequently found to be an effective treatment for OUD, decreasing opioid withdrawal and craving, illicit opioid use, and mortality.4,5,6,7 The passage of the Drug Addiction Treatment Act (DATA) of 2000 allowed for buprenorphine to be prescribed in outpatient settings for treatment of OUD.3 There are now several formulations of buprenorphine approved by the FDA for OUD and chronic pain. Sublingual (brand names Subutex [buprenorphine alone], Suboxone or Zubsolv [buprenorphine-naloxone]), injectable (Sublocade), and implantable (Probuphine) preparations are FDA-approved for OUD only. Buccal (Bunavail) and transdermal (Butrans) formulations are FDA-approved for treatment of chronic pain. Sublingual buprenorphine has also been used for off-label treatment of chronic pain,8 particularly in those with chronic pain who develop higher risk prescription opioid use9, 10 and for those in whom the pain-approved formulations are of inadequate analgesic dose.
While its high binding affinity to the mu-opioid receptor and long half-life make it ideal for treatment of OUD, there is concern among clinicians that buprenorphine will prevent effective analgesia if other opioids are required for the management of acute pain due to surgery, injury, or acute illness. The following are two typical scenarios that might be encountered by the general practitioner in clinical practice:
-
Case 1: A 24-year-old patient with OUD, stable on buprenorphine-naloxone 12–3 mg SL twice daily, is scheduled for dental extraction. Should the patient continue on buprenorphine on the day of the procedure and how should pain be managed after the procedure?
-
Case 2: A 36-year-old patient with OUD, on buprenorphine-naloxone 8–2 mg SL twice daily, is admitted for right foot osteomyelitis with overlying soft tissue infection. Orthopedic surgery recommends surgical debridement. The patient is currently experiencing severe pain. How should the patient’s acute pain and postoperative pain be managed?
There is still mixed guidance in literature on how to manage buprenorphine perioperatively, with some guidance (particularly in anesthesia literature) recommending that patients taper off or stop buprenorphine preoperatively, particularly in cases where moderate to severe pain is expected.11,12,13,14 In our clinical experience, some practitioners still ask patients to taper off buprenorphine up to 2 weeks prior to planned surgery. However, among all patients with OUD treated with buprenorphine, those who are tapered off rather than maintained on buprenorphine have been found to be at higher risk of relapse and overdose.15 This increased risk of relapse, as well as the difficulty of transitioning back of buprenorphine postoperatively, has led many, including SAMHSA and the American Society of Addiction Medicine (ASAM), to question the routine practice of perioperative buprenorphine dose disruption.16, 17 The purpose of this narrative review is to summarize the existing literature for acute pain and perioperative management in patients treated with buprenorphine for OUD and to provide practical recommendations regarding perioperative pain management for the general practitioner based on evidence and clinical experience.
Pharmacology of Buprenorphine
Properties at Mu-Opioid Receptor
Mu Receptor Agonist Properties
Buprenorphine is a semi-synthetic partial (low intrinsic efficacy) agonist at the mu-opioid receptor, which mediates effects on opioid craving and withdrawal, analgesia, and respiratory depression. Given its partial agonism, the maximum analgesic effect produced by buprenorphine is less than that produced by a full agonist opioid, particularly in patients with opioid tolerance.18 Sublingual doses of 16 mg occupy 79 to 95% of mu-opioid receptors, and doses greater than 24 to 32 mg occupy up to 95% occupancy of receptors.19 While earlier studies showed ceiling effect for respiratory depression,20 a recent systematic review of 28 randomized controlled studies involving 2210 patients comparing buprenorphine and morphine in acute pain management showed no difference in pain, respiratory depression, or sedation.21
Mu Receptor Affinity
Buprenorphine has a higher binding affinity at the mu receptor than other opioids: 1.7 times that of hydromorphone, 5.4 times that of morphine, 6.2 times that of fentanyl, and 120 times that of oxycodone.22 This high affinity means that when buprenorphine is administered too soon after full agonist opioids, it will competitively displace them from the mu receptor, leading to a precipitated withdrawal.23 Precipitated withdrawal can be avoided by waiting to administer buprenorphine until the patient develops symptoms of opioid withdrawal (a sign of low receptor occupancy). Buprenorphine’s high binding affinity has led to the misperception among many clinicians that it is impossible to treat perioperative pain in patients treated with buprenorphine maintenance. However, receptor theory and clinical observations have shown that this blockade can be overridden with higher doses of full agonist opioids.24, 25 In a study by Mercadante et al. of 29 patients with chronic cancer pain on transdermal buprenorphine, all acute pain events were successfully managed with IV morphine without discontinuing buprenorphine.26
Mu Receptor Dissociation
Buprenorphine has slow dissociation kinetics (approximately 166 min),27 contributing to its long half-life and allowing for once or twice daily dosing in maintenance therapy for OUD. The half-life for transmucosal buprenorphine is variable and ranges from 24–42 h (based on package inserts), with broad interpatient half-life variability (24 to 60 h).18 Half-life for transmucosal preparations is longer than for intravenous (IV) ones (3 h), possibly due to sequestration in the oral mucosa and lipid storage sites when administered transmucosally.28 In general, the analgesic half-life is shorter than the half-life of the drug, such that three or four times daily dosing is often preferable for analgesia.29
Kappa, Delta, and ORL-1 Receptor Antagonism
Buprenorphine and its active metabolite norbuprenorphine have both agonist and antagonist properties at the kappa- and delta-opioid receptors and ORL-1 receptor.30 Kappa-opioid antagonism is thought to contribute to some of the reversal of opioid-induced hyperalgesia with buprenorphine noted in preliminary studies.31 ORL-1 effects at higher doses may be an important mediator of buprenorphine’s ceiling effect in vivo.30, 32
Review of Original Research
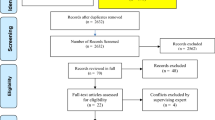
For this narrative review, a selection of relevant research studies is summarized in the following section to provide insight into changing practices regarding perioperative buprenorphine management and serve as a foundation for management decisions for the general practitioner. The authors used PubMed to identify English-language articles related to buprenorphine, OUD, and perioperative management including case studies, comparative studies, and review articles. Articles were selected based on expert opinion regarding relevance to the general practitioner. Given limited studies specifically comparing perioperative cessation and continuation of buprenorphine for patients with OUD, literature was also included that compared patients maintained on buprenorphine with opioid-naive or methadone-maintained controls.
Perioperative Pain Management in Patients on Buprenorphine
Tables 1 and 2 summarize the existing literature on perioperative pain management of patients on buprenorphine. Nine case reports33,34,35,36,37,38,39,40,41 and two case series,42, 43 comprising a total of 17 cases, were identified that described perioperative course or pain management after traumatic injury among patients treated with buprenorphine for chronic pain or OUD (Table 2). In 12 of the 15 cases where buprenorphine was continued (5 case reports, plus 8 cases from the 2 case series), adequate pain control was achieved.33, 38, 41,42,43 Discontinuing buprenorphine was only required in three of the cases.36, 39, 40 Of note, pain control in these patients required multi-modal management and titration of medication, including regional pain blocks35 and adjustment of buprenorphine dose.38 In the two cases where buprenorphine was discontinued 3–5 days preoperatively, it was difficult to achieve adequate pain control in the perioperative period.34, 37 Many of the patients in these cases were noted to require high doses of opioids (with or without buprenorphine), which is consistent with known opioid tolerance among patients with OUD.
Five studies compared the adequacy of postoperative pain control in patients maintained on baseline buprenorphine versus other patient populations (Table 2). Two of the five studies retrospectively evaluated pain care outcomes in pregnant women maintained on buprenorphine44 or methadone45 for OUD compared with opioid-naive controls. Meyer et al. found no difference in intrapartum pain control or efficacy of regional anesthesia between pregnant women continued on their baseline buprenorphine through delivery compared with matched opioid-naive controls. Among patients treated with buprenorphine maintenance, they found mildly higher pain scores without increased opioid use after vaginal delivery and higher pain scores with 47% increase in opioid use after delivery by cesarean section.44 However, Hoflich et al. found no difference in post-partum pain control after vaginal delivery, and increased non-steroidal anti-inflammatory drug (NSAID) use with decreased opioid use after cesarean section among patients maintained on buprenorphine or methadone compared with opioid-naive controls. They found that patients receiving buprenorphine or methadone required epidural anesthesia more often during vaginal delivery but this was accounted for by differences in smoking status between the two groups in regression analyses.45 Prior literature has suggested that chronic nicotine use may reduce mu-opioid receptor availability resulting in greater difficulty controlling pain.46 These studies suggest that maintenance of buprenorphine does not introduce significant complications to pain control after vaginal or cesarean delivery compared with those unexposed to opioids.
Three additional studies compared analgesic requirements of patients with OUD on buprenorphine to those on methadone undergoing surgery,47 vaginal delivery,48 or C-section.49 In two of these studies, all participants were continued on their maintenance therapy through the perioperative/peripartum periods. Jones et al. found that, after vaginal delivery, there was no significant difference in pain ratings (which were in the mild range), use of acetaminophen, or use of oxycodone between patients continued on buprenorphine and those on methadone; patients on buprenorphine used less ibuprofen than those on methadone.48 Similarly, Vilkins et al. found adequate pain control and no significant differences in opioid requirements between patients maintained on buprenorphine and methadone after delivery by cesarean section.49 These studies suggest that similar pain management strategies can be used for patients with OUD on methadone and buprenorphine.
Macintyre et al. performed a retrospective analysis of patients on baseline buprenorphine and methadone, some of whom had their doses held and some of whom had their doses continued on the day of and day after surgery.47 They found no correlation between PCA-based opioid requirement in the first 24 h after surgery and the preoperative dose of either buprenorphine or methadone. Additionally, patients who did not receive their buprenorphine dose on the day after surgery required longer duration of PCA and supervision by the pain medicine service and had higher opioid requirements than those who did. Of note, there were no differences in opioid requirement between those who did versus those who did not receive their baseline methadone on the day after surgery.
Current Practice Recommendations and Controversies
In the absence of sufficient data, there has been a lack of consensus on the best approach to perioperative management of patients maintained on buprenorphine.11, 50,51,52 As such, existing recommendations on perioperative management of buprenorphine-maintained patients have largely arisen out of expert opinion based on the pharmacologic principles of buprenorphine, case reports, and clinical experience. The recommendations often differ based on the type of surgery (e.g., emergent vs. elective), the degree of anticipated postoperative pain, the patient’s baseline dose, and the age of the publication. In general, earlier publications often recommend discontinuation of buprenorphine for elective procedures, citing concerns for a ceiling effect of buprenorphine’s analgesic properties and inability to achieve sufficient analgesia from full agonist opioids due to buprenorphine’s high affinity for the receptor and the potential for competition at the mu-opioid receptor.50, 51 However, in response to emerging evidence of ability to achieve sufficient analgesia in buprenorphine-maintained patients (reviewed above) as well as concerns of predisposing patients with OUD to an increased risk of relapse and overdose with discontinuation of buprenorphine—particularly when exposing them to full agonist opioids used for acute pain care—continuation of buprenorphine in the perioperative period is increasingly common in clinical practice and recent publications.
Variability remains with respect to the circumstances under which discontinuation of buprenorphine is discouraged or recommended, as well as the timing of discontinuation. Some authors recommend continuation of buprenorphine for anticipated minimal to mild pain, but discontinuation of buprenorphine and transition to short-acting full agonist opioids in situations where moderate to severe pain is anticipated.11, 12, 18, 53 In contrast, many clinicians and several authors have recommended continuing buprenorphine without interruption regardless of severity of expected pain, including administration of the maintenance dose on the morning of the surgery and continuation postoperatively.13, 14, 41, 54 However, among those authors and institutional guidelines that recommend continuation of buprenorphine, there remains variability in recommendations regarding the maximum dose of buprenorphine that should be given. For example, in their 2005 paper, Roberts and Meyer-Witting recommend increasing the buprenorphine dose by 25% for major surgeries.55 Conversely, a recent editorial by Lembke and colleagues recommends that those patients on buprenorphine doses higher than 12 mg be tapered down to 12 mg in the 2–3 days prior to surgery, with return to the maintenance dose as early as 3 days postoperatively.52 A recent review from Quaye and Zhang recommends continuing home buprenorphine dose for minor procedures and decreasing buprenorphine to 8 mg sublingual daily for major procedures.56 The authors of these articles consistently recommend continuation of buprenorphine through perioperative period and management of breakthrough acute pain with multi-modal approaches, including as-needed full agonist opioids, as well as non-pharmacologic options, non-opioid medications, and regional anesthesia.
Summary and Recommendations
In our clinical experience as addiction medicine and pain specialists, in cases in which buprenorphine is stopped preoperatively, patients are typically discharged from the hospital on full agonist opioids alone, requiring re-initiation of buprenorphine in the outpatient setting, which is challenging for the patients and puts them at high risk of relapse. In contrast, patients with OUD on buprenorphine maintenance do best when buprenorphine is continued through the perioperative period and a multi-modal approach to acute breakthrough pain is utilized. Based on the previously presented literature and our clinical expertise, we make the following recommendations:
Continue buprenorphine in the perioperative period for patients with OUD who are on buprenorphine
Based on expert consensus, SAMHSA updated its guidelines in 2018 to recommend that most patients continue buprenorphine through the perioperative period due to increased risk of relapse when it is discontinued.17 A recent review of literature supports continuation of buprenorphine56 and clinical protocols at many leading US medical centers are now reflecting this approach.52, 57 While more research is needed, our recommendation is to continue buprenorphine through the perioperative period, including in peripartum management in obstetrical populations, regardless of whether additional full agonist opioids are needed. In our clinical practice, we continue buprenorphine without dose reduction (similar to management of methadone); however, further research is needed on optimal dose of buprenorphine in the perioperative period. As buprenorphine formulations are either sublingual, buccal, transdermal, or implantable, there is no need to hold this medication while a patient is NPO either pre- or postoperatively.
Use a multi-modal analgesic approach
An effective analgesic plan requires a multi-modal approach, inclusive of appropriate anesthesiology techniques (e.g., regional anesthesia); non-pharmacologic interventions; non-opioid analgesics; and, when appropriate, short-acting opioid analgesics. Non-opioid modalities should be used to reduce opioid requirements in the perioperative period. Non-opioid medications with pain modulating properties, including NSAIDs, acetaminophen, duloxetine,58 gabapentinoids, ketamine, IV lidocaine, and alpha-agonists, such as clonidine, prazosin, and dexmetomidine,59 have been shown to be effective as opioid-sparing approaches during the postoperative period. Continuous regional/neuraxial blocks have been utilized successfully for the relief of severe postoperative pain.60 Mind-body therapies, such as mindfulness meditation and hypnotic suggestion, have been shown to decrease pain in hospitalized patients by up to 29% right after the practice.61 Patients can be safely discharged on oral non-opioid analgesic medications for ongoing postoperative pain. NSAIDs, acetaminophen, and duloxetine have good safety profiles and low risk for abuse and are preferred medications for discharge. Gabapentinoids have more potential for abuse, particularly in patients with substance use disorders, and should be used with caution.62
As part of a multi-modal approach, buprenorphine and short-acting full agonists can also be utilized for pain control. Given the shorter analgesic half-life of buprenorphine, a patient’s total daily dose (TDD) can be divided into three to four times daily dosing for better analgesic effect. In addition, the buprenorphine TDD can be increased in cases of mild pain (pain score less than 4). Patients with moderate to severe pain (pain score greater than 5) will likely need short-acting full agonist opioids in the immediate postoperative period. In these cases, continue the patient’s home buprenorphine dose and select one short-acting full agonist (either PO or IV, depending on pain severity), reassessing the patient’s response after each dose and titrating as needed. Consider transition to IV PCA if pain cannot be controlled with PO or IV options (PCA settings should include boluses only, as the patient’s baseline buprenorphine should take the place of a basal infusion). Notably, starting doses of short-acting full agonists will be higher than those required for an opioid-naive patient (ex. oxycodone 10–15 mg by mouth every 4–6 h rather than 5 mg; see Table 3 for detailed recommendations). Decisions about discharging a patient on full agonist opioids should be individualized, with consideration of expected duration of acute pain and patient stability and ability to safely take opioids as prescribed; these decisions should be communicated to the patient’s outpatient buprenorphine prescriber to improve continuity of care. In our practice, we generally discharge patients requiring ongoing full-agonist opioids with 1–2-week supply of medication, plan for taper, and close follow-up with outpatient provider.
Care coordination and discharge planning are essential components of an effective perioperative analgesic plan for patients with OUD treated with buprenorphine
We recommend multi-disciplinary care coordination, inclusive of collaboration with the outpatient buprenorphine prescriber and, when possible, expert consultation from addiction medicine and/or anesthesia/pain medicine colleagues. Finally, for elective surgeries, we recommend preoperative patient assessment with development of the planned intraoperative and postoperative analgesic approaches and post-discharge planning.
An individualized approach to perioperative pain management should be based on shared decision-making
There are many factors influencing perioperative pain management that vary between patients, including stability on buprenorphine treatment, pain tolerance, preference for pain modalities, and degree of psychosocial support. With the above three recommendations as a guide, decisions regarding perioperative pain management should be individualized and based on shared-decision making between the patient and provider.
The cases are revisited below as illustrations of our approach to management of buprenorphine when there is acute pain due to surgery, injury, or acute illness, including when and how to use additional short-acting full agonist opioids. Table 3 includes a summary of general management principles applicable to each case.
Case 1—Mild Pain or Minor Procedure
A 24-year-old patient with OUD, stable on buprenorphine-naloxone 12–3 mg SL twice daily, is scheduled for dental extraction.
Recommendation:
-
Continue home buprenorphine without dose reduction and advise patient to take NSAIDs (such as ibuprofen 800 mg three times daily) and acetaminophen 500–1000 mg three times daily for pain. The dentist can use local anesthesia for this routine dental procedure.
-
If patient reports inadequate pain relief, buprenorphine dose can be split into 6 mg (1/2 film or tab) four times daily.
Case 2—Severe Pain or Major Procedure
A 36-year-old patient with OUD, on buprenorphine-naloxone 8–2 mg SL twice daily, has severe pain from osteomyelitis with overlying soft tissue infection, awaiting surgical debridement.
Recommendation:
-
Continue home buprenorphine 8 mg SL twice daily for opioid dependence, including on the day of surgical debridement. After surgery, dosing can be split into 4 mg SL four times daily if needed.
-
Start around-the-clock NSAIDs and acetaminophen, per above dosing, for baseline pain control. For severe pain, start short-acting full agonist opioid such as oxycodone or hydromorphone (e.g., start with oxycodone 10–15 mg PO every 4 h or hydromorphone 4–6 mg PO every 4 h as needed). Re-assess after each dose to determine if pain control is adequate and increase dose until pain is tolerable.
-
Strongly consider consulting anesthesia/pain medicine for initiation of a regional block of the affected limb.
Thoughtful management of acute perioperative pain among patients on buprenorphine for OUD is of critical importance, given the risks of destabilization during the perioperative period. Maintaining buprenorphine and utilizing an individualized, multi-modal, and multi-disciplinary approach to analgesia are key components of a successful strategy. Notably, this field of knowledge, at the intersection of addiction medicine, pain medicine, and anesthesia, is rapidly evolving with wide variability in practice. More research, particularly on such topics as ideal perioperative buprenorphine dosing and the most effective modes of non-opioid analgesia in this population, is needed to further optimize perioperative strategies for acute pain management for patients with OUD maintained on buprenorphine.
References
SAMHSA. Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Survey on Drug Use and Health (HHS Publication No. SMA 18-5068, NSDUH Series H-53). Rockville, MD; 2018.
Hedegaard H, Miniño AM, Warner M. Drug Overdose Deaths in the United States, 1999-2017. NCHS Data Brief. 2018;(329):1-8.
Johnson RE, Fudala PJ, Payne R. Buprenorphine: Considerations for pain management. J Pain Symptom Manage. 2005;29(3):297-326.
Cornish R, Macleod J, Strang J, Vickerman P, Hickman M. Risk of death during and after opiate substitution treatment in primary care: prospective observational study in UK General Practice Research Database. BMJ. 2010;341:c5475.
Fudala PJ, Bridge TP, Herbert S, et al. Office-Based Treatment of Opiate Addiction with a Sublingual-Tablet Formulation of Buprenorphine and Naloxone. N Engl J Med. 2003;349(10):949-958.
Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;(2):1-85.
Schackman BR, Leff JA, Polsky D, Moore BA, Fiellin DA. Cost-effectiveness of long-term outpatient buprenorphine-naloxone treatment for opioid dependence in primary care. J Gen Intern Med. 2012;27(6):669-676.
Roux P, Sullivan MA, Cohen J, et al. Buprenorphine/naloxone as a promising therapeutic option for opioid abusing patients with chronic pain: Reduction of pain, opioid withdrawal symptoms, and abuse liability of oral oxycodone. Pain. 2013;154(8):1442-1448.
Blondell RD, Ashrafioun L, Dambra CM, Foschio EM, Zielinski AL, Salcedo DM. A Clinical Trial Comparing Tapering Doses of Buprenorphine with Steady Doses for Chronic Pain and Co-existent Opioid Addiction. J Addict Med. 2010;4(3):140-146.
Malinoff HL, Barkin RL, Wilson G. Sublingual buprenorphine is effective in the treatment of chronic pain syndrome. Am J Ther. 12(5):379-384.
Jonan AB, Kaye AD, Urman RD. Buprenorphine Formulations: Clinical Best Practice Strategies Recommendations for Perioperative Management of Patients Undergoing Surgical or Interventional Pain Procedures. Pain Physician. 2018;21:E1-E12.
Childers J, Arnold R. Treatment of Pain in Patients Taking Buprenorphine. J Palliat Med. 2012;15:613-614.
Mehta V, Langford RM. Acute pain management for opioid dependent patients. Anaesthesia. 2006;61:269-276.
Ward EN, Quaye AN-A, Wilens TE. Opioid Use Disorders: Perioperative Management of a Special Population. Anesth Analg. 2018;127(2):539-547.
Williams AR, Samples H, Crystal S, Olfson M. Acute Care, Prescription Opioid Use, and Overdose Following Discontinuation of Long-Term Buprenorphine Treatment for Opioid Use Disorder. Am J Psychiatry. 2020;177(2):117-124.
ASAM. The ASAM National Practice Guideline for the Treatment of Opioid Use Disorder: 2020 Focused Update. J Addict Med. 2020;14(2S):1-91.
SAMHSA. Medications for Opioid Use Disorder. Treatment Improvement Protocol (TIP) Series 63, Full Document. HHS Publication No. (SMA) 19-5063FULLDOC. Rockville, MD; 2018.
Anderson TA, Quaye ANA, Ward EN, Wilens TE, Hilliard PE, Brummett CM. To Stop or Not, That Is the Question. Anesthesiology. 2017;126(6):1180-1186.
Greenwald MK, Johanson CE, Moody DE, et al. Effects of Buprenorphine Maintenance Dose on μ-Opioid Receptor Availability, Plasma Concentrations, and Antagonist Blockade in Heroin-Dependent Volunteers. Neuropsychopharmacology. 2003;28(11):2000-2009.
Dahan A, Yassen A, Romberg R, et al. Buprenorphine induces ceiling in respiratory depression but not in analgesia. Br J Anaesth. 2006;96(5):627-632.
White LD, Hodge A, Vlok R, Hurtado G, Eastern K, Melhuish TM. Efficacy and adverse effects of buprenorphine in acute pain management: systematic review and meta-analysis of randomised controlled trials. Br J Anaesth. 2018;120(4):668-678.
Volpe DA, Tobin GAM, Mellon RD, et al. Uniform assessment and ranking of opioid Mu receptor binding constants for selected opioid drugs. Regul Toxicol Pharmacol. 2011;59(3):385-390.
Coe MA, Lofwall MR, Walsh SL. Buprenorphine Pharmacology Review. J Addict Med. 2019;13(2):93-103. https://doi.org/10.1097/ADM.0000000000000457
Bickel WK, Stitzer ML, Bigelow GE, Liebson IA, Jasinski DR, Johnson RE. Buprenorphine: dose-related blockade of opioid challenge effects in opioid dependent humans. J Pharmacol Exp Ther. 1988;247(1):47-53.
Strain EC, Walsh SL, Bigelow GE. Blockade of hydromorphone effects by buprenorphine/naloxone and buprenorphine. Psychopharmacology (Berl). 2002;159(2):161-166.
Mercadante S, Villari P, Ferrera P, et al. Safety and Effectiveness of Intravenous Morphine for Episodic Breakthrough Pain in Patients Receiving Transdermal Buprenorphine. J Pain Symptom Manage. 2006;32(2):175-179.
Boas RA, Villiger JW. Clinical Actiions of Fentanyl and Buprenorphine: The Significance of Receptor Binding. Br J Anaesth. 1985;57(2):192-196.
Welsh C, Valadez-Meltzer A. Buprenorphine: A (Relatively) New Treatment For Opioid Dependence. Psychiatry (Edgmont). 2005;2(12):29-39.
Vadivelu N, Mitra S, Kaye AD, Urman RD. Perioperative analgesia and challenges in the drug-addicted and drug-dependent patient. Best Pract Res Clin Anaesthesiol. 2014;28(1):91-101. https://doi.org/10.1016/j.bpa.2014.02.003
Lutfy K, Eitan S, Bryant CD, et al. Buprenorphine-Induced Antinociception Is Mediated by μ-Opioid Receptors and Compromised by Concomitant Activation of Opioid Receptor-Like Receptors. J Neurosci. 2003;23(32):10331-10337.
Chen KY, Chen L, Mao J. Buprenorphine–Naloxone Therapy in Pain Management. Anesthesiology. 2014;120:1262-1274.
Lutfy K, Cowan A. Buprenorphine: a unique drug with complex pharmacology. Curr Neuropharmacol. 2004;2(4):395-402.
Book SW, Myrick H, Malcolm R, Strain EC. Buprenorphine for Postoperative Pain Following General Surgery in a Buprenorphine-Maintained Patient. Am J Psychiatry. 2007;164(6):979.
Chern S-YS, Isserman R, Chen L, Ashburn M, Liu R. Perioperative Pain Management for Patients on Chronic Buprenorphine: A Case Report. J Anesth Clin Res. 2013;3(250).
Gilmore T, Saccheti A, Cortese T. Buprenorphine/naloxone inhibition of remifentanil procedural sedation. Am J Emerg Med. 2012;30(8):2009-2010.
Harrington CJ, Zaydfudim V. Buprenorphine maintenance therapy hinders acute pain management in trauma. Am Surg. 2010;76(4):397-399.
Israel JS, Poore SO. The Clinical Conundrum of Perioperative Pain Management in Patients with Opioid Dependence: Lessons from Two Cases. Plast Reconstr Surg. 2011;127:2141-2150.
Huang A, Katznelson R, de Perrot M, Clarke H. Gestion périopératoire d’un patient subissant la fermeture d’une fenêtre de Clagett stabilisé par Suboxone® pour douleur chronique: une étude de cas. Can J Anesth. 2014;61(9):826-831.
Khelemsky Y, Schauer J, Loo N. Effect of Buprenorphine on Total Intravenous Anesthetic Requirements During Spine Surgery. Pain Physician. 2015;18:E261-E264.
McCormick Z, Chu SK, Chang-Chien GC, Joseph P. Acute Pain Control Challenges with Buprenorphine/Naloxone Therapy in a Patient with Compartment Syndrome Secondary to McArdle’s Disease: A Case Report and Review. Pain Med. 2013;14(8):1187-1191.
Silva MJ, Rubinstein A. Continuous Perioperative Sublingual Buprenorphine. J Pain Palliat Care Pharmacother. 2016;30(4):289-293.
Kornfeld H, Manfredi L. Effectiveness of Full Agonist Opioids in Patients Stabilized on Buprenorphine Undergoing Major Surgery- A Case Series. Am Jounral Ther. 2010;17:523-528.
Leighton BL, Crock LW. Case Series of Successful Postoperative Pain Management in Buprenorphine Maintenance Therapy Patients. Anesth Analg. 2017;125(5):1779-1783.
Meyer M, Paranya G, Keefer Norris A, Howard D. Intrapartum and postpartum analgesia for women maintained on buprenorphine during pregnancy. Eur J Pain. 2010;14:939-943.
Höflich AS, Langer M, Jagsch R, et al. Peripartum pain management in opioid dependent women. Eur J Pain. 2012;16(4):574-584.
Greenwald MK, Comer SD, Fiellin DA. Buprenorphine maintenance and mu-opioid receptor availability in the treatment of opioid use disorder: implications for clinical use and policy. Drug Alcohol Depend. 2014;144:1-11.
Macintyre P, Russell R, Usher K, Gaughwin M, Hutable C. Pain Relief and Opioid Requirements in the First 24hrs After Surgery in Patients Taking Buprenorphine and Methadone Opioid Substitution Therapy. Anaesth Intensive Care. 2013;41(2):222-230.
Jones HE, O’Grady K, Dahne J, et al. Management of acute postpartum pain in patients maintained on methadone or buprenorphine during pregnancy. Am J Drug Alcohol Abuse. 2009;35(3):151-156.
Vilkins AL, Bagley SM, Hahn KA, et al. Comparison of Post-Cesarean Section Opioid Analgesic Requirements in Women with Opioid Use Disorder Treated with Methadone or Buprenorphine. J Addict Med. 2017;11:397-401.
Alford DP, Compton P, Samet JH. Acute Pain Management for Patients Receiving Maintenance Methadone or Buprenorphine Therapy. Ann Intern Med. 2006;144:127-134.
Bryson EO. The perioperative management of patients maintained on medications used to manage opioid addiction. Curr Opin Anaesthesiol. 2014;27:359-364.
Lembke A, Ottestad E, Schmiesing C. Patients Maintained on Buprenorphine for Opioid Use Disorder Should Continue Buprenorphine Through the Perioperative Period. Pain Med. 2019;20(3):425-428.
Sen S, Arulkumar S, Cornett EM, et al. New Pain Management Options for the Surgical Patient on Methadone and Buprenorphine. Curr Pain Headache Rep. 2016;20:1-8.
Warltier DC, Mitra S, Sinatra RS. Perioperative Management of Acute Pain in the Opioid- dependent Patient. Anesthesiology. 2004;101:212-227.
Roberts DM, Meyer-Witting M. High-dose buprenorphine: Perioperative precautions and management strategies. Anaesth Intensive Care. 2005;33:17-25.
Quaye AN-A, Zhang Y. Perioperative Management of Buprenorphine: Solving the Conundrum. Pain Med. 2019;20(7):1395-1408.
Johns Hopkins Division of Addiction Medicine. Recommendations for Management of Acute Pain for Patients on Medications for Opioid Use Disorder (mOUD) Presenting to ED and Inpatient Settings. 2019.
Castro-Alves LJ, Oliveira de Medeiros ACP, Neves SP, et al. Perioperative Duloxetine to Improve Postoperative Recovery After Abdominal Hysterectomy: A Prospective, Randomized, Double-Blinded, Placebo-Controlled Study. Anesth Analg. 2016;122(1):98-104.
Ramaswamy S, Wilson JA, Colvin L. Non-opioid-based adjuvant analgesia in perioperative care. Contin Educ Anaesth Crit Care Pain. 2013;13(5):152-157.
Suksompong S, von Bormann S, von Bormann B. Regional Catheters for Postoperative Pain Control: Review and Observational Data. Anesthesiol Pain Med. 2020;10(1). https://doi.org/10.5812/aapm.99745
Garland EL, Baker AK, Larsen P, et al. Randomized Controlled Trial of Brief Mindfulness Training and Hypnotic Suggestion for Acute Pain Relief in the Hospital Setting. J Gen Intern Med. 2017;32(10):1106-1113.
Smith R V., Havens JR, Walsh SL. Gabapentin misuse, abuse and diversion: a systematic review. Addiction. 2016;111(7):1160-1174. https://doi.org/10.1111/add.13324
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Buresh, M., Ratner, J., Zgierska, A. et al. Treating Perioperative and Acute Pain in Patients on Buprenorphine: Narrative Literature Review and Practice Recommendations. J GEN INTERN MED 35, 3635–3643 (2020). https://doi.org/10.1007/s11606-020-06115-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-020-06115-3