
Abstract
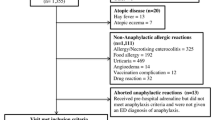
Despite multiple recommendations, intramuscular epinephrine is poorly prescribed in emergency department receiving pediatric anaphylaxis. To evaluate the role of severity symptoms on this use, we included all admissions for a diagnosis linked to possible allergy in the two pediatric emergency departments of our institution between January 2010 and December 2015. Selection and analysis were restricted to children under 18 years fulfilling Sampson’s criteria for anaphylaxis. We retrospectively ranked these admissions with the Ring and Messmer anaphylaxis severity score and compared the use of epinephrine according to this classification. Among 422,483 admissions, 204 (0.05%) fulfilled the anaphylaxis criteria (170 (83.3%) grade II anaphylaxis, and 34 (16.7%) grade III; mean age 7.9 years). Previous allergy, anaphylaxis, and asthma were found in respectively 60.8%, 36.8%, and 35.1%. Food allergy was the main suspected causal trigger. Epinephrine was used in 32.7% (n = 65/199), before admission (11.4% (n = 23/201)) or in the emergency department (22.2% (n = 45/202)). Epinephrine was more frequently prescribed in grade III than in grade II anaphylaxis (84.8% vs 22.3%, p < 0.001; OR = 19.05 [7.05–54.10]). Upon discharge, epinephrine auto-injectors prescription and allergy referral were rare (31.7% and 44.2%).
Conclusion: Pediatricians intuitively adapt their epinephrine use to the severity of the anaphylaxis and contribute to epinephrine underuse in pediatric anaphylaxis.
What is known: • Intramuscular epinephrine is the recommended treatment for pediatric anaphylaxis. However, most of the European and North-American studies show a low prescription rate of epinephrine in both prehospital and pediatric emergency department management. • Reasons for such a low prescription rate are unknown. | |
What is new: • This study confirms that intramuscular epinephrine is poorly prescribed in pediatric anaphylaxis (about one case among 10 before admission and one among 5 in pediatric emergency departments). • Despite recommendations, pediatricians intuitively adapt their prescription to the clinical severity of anaphylaxis, with a fourfold increase prescription in grade III compared to grade II anaphylaxis. This medical behavior ascertainment may be in part explained by the delay between the ED admission/management and the anaphylactic episode onset. |

Similar content being viewed by others

References
Alonso T, Moro Moro M, García M (2015) Epidemiology of anaphylaxis. Clin Exp Allergy 45:1027–1039
Andrew E, Nehme Z, Bernard S, Smith K (2018) Pediatric anaphylaxis in the prehospital setting: incidence, characteristics, and management. Prehosp Emerg Care 19:1–7
Ben-Shoshan M, Clarke AE (2011) Anaphylaxis: past, present and future. Allergy 66:1–14
Brown JC, Tuuri RE, Akhter S, Guerra LD, Goodman IS, Myers SR, Nozicka C, Manzi S, Long K, Turner T, Conners GP, Thompson RW, Park E (2016) Lacerations and embedded needles caused by epinephrine autoinjector use in children. Ann Emerg Med 67:307–315
Cardona V, Ferré-Ybarz L, Guilarte M, Moreno-Pérez N, Gómez-Galán C, Alcoceba-Borràs E, Delavalle MB, Garriga-Baraut T, on behalf of the AdreSCAIC Research Group (2017) Safety of adrenaline use in anaphylaxis: a multicenter register. Int Arch Allergy Immunol 173:171–177
Carrillo E, Hern HG, Barger J (2016) Prehospital administration of epinephrine in pediatric anaphylaxis. Prehosp Emerg Care 20:239–244
de Silva IL, Mehr SS, Tey D, Tang ML (2008) Paediatric anaphylaxis: a 5 year retrospective review. Allergy 63:1071–1076
Farbman KS, Michelson KA (2016) Anaphylaxis in children. Curr Opin Pediatr 28:294–297
Farbman KS, Michelson KA, Neuman MI, Dribin TE, Schneider LC, Stack AM (2017) Reducing hospitalization rates for children with anaphylaxis. Pediatrics 139:e20164114
Ganapathy S, Lwin Z, Ting DH, Goh LS, Chong SL (2016) Anaphylaxis in children: experience of 485 episodes in 1,272,482 patient attendances at a tertiary paediatric emergency department from 2007 to 2014. Ann Acad Med Singap 45:542–548
Grabenhenrich LB, Dölle S, Moneret-Vautrin A, Köhli A, Lange L, Spindler T, Ruëff F, Nemat K, Maris I, Roumpedaki E, Scherer K, Ott H, Reese T, Mustakov T, Lang R, Fernandez-Rivas M, Kowalski ML, Bilò MB, Hourihane JO'B, Papadopoulos NG, Beyer K, Muraro A, Worm M (2016) Anaphylaxis in children and adolescents: the European anaphylaxis registey. J Allergy Clin Immunol 137:1128–1137
Hochstadter E, Clarke A, De Schryver S et al (2016) Increasing visits for anaphylaxis and the benefits of early epinephrine administration: a 4-year study at a pediatric emergency department in Montreal, Canada. J Allergy Clin Immunol 137:1888–1890
Huang F, Chawla K, Järvinen KM, Nowak-Wegrzyn A (2012) Anaphylaxis in a New York City pediatric emergency department: triggers, treatments, and outcomes. J Allergy Clin Immunol 129:162–168
Manuyakorn W, Benjaponpitak S, Kamchaisatian W, Vilaiyuk S, Sasisakulporn C, Jotikasthira W (2015) Pediatric anaphylaxis: triggers, clinical features, and treatment in a tertiary-care hospital. Asian Pac J Allergy Immunol 33:281–288
Michelson KA, Monuteaux MC, Neuman MI (2016) Variation and trends in anaphylaxis care in United States children’s hospitals. Acad Emerg Med 23:623–627
Muraro A, Roberts G, Worm M, Bilò MB, Brockow K, Fernández Rivas M, Santos AF, Zolkipli ZQ, Bellou A, Beyer K, Bindslev-Jensen C, Cardona V, Clark AT, Demoly P, Dubois AEJ, DunnGalvin A, Eigenmann P, Halken S, Harada L, Lack G, Jutel M, Niggemann B, Ruëff F, Timmermans F, Vlieg-Boerstra BJ, Werfel T, Dhami S, Panesar S, Akdis CA, Sheikh A, the EAACI Food Allergy and Anaphylaxis Guidelines Group (2014) Anaphylaxis: guidelines from the European academy of allergy and clinical immunology. Allergy 69:1026–1045
O’Keefe A, Clarke A, St Pierre Y et al (2017) The risk of recurrent anaphylaxis. J Pediatr 180:217–221
Pouessel G, Galand J, Beudouin E et al (2017) The gaps in anaphylaxis diagnosis and management by French physicians. Pediatr Allergy Immunol 28:295–298
Pouessel G, Tanno LK, Claverie C, Lejeune S, Labreuche J, Dorkenoo A, Renaudin JM, Eb M, Leteurtre S, Deschildre A (2018) Fatal anaphylaxis in children in France: analysis of national data. Pediatr Allergy Immunol 29:101–104
Ring J, Messmer K (1997) Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet 309:466–469
Robinson M, Greenhawt M, Stukus DR (2017) Factors associated with epinephrine administration for anaphylaxis in children before arrival to the emergency department. Ann Allergy Asthma Immunol 119:164–169
Russell S, Monroe K, Losek JD (2010) Anaphylaxis management in the pediatric emergency department: opportunities for improvement. Pediatr Emerg Care 26:71–76
Sampson HA, Muñoz-Furlong A, Campbell RL, Adkinson NF Jr, Bock SA, Branum A, Brown SGA, Camargo CA Jr, Cydulka R, Galli SJ, Gidudu J, Gruchalla RS, Harlor AD Jr, Hepner DL, Lewis LM, Lieberman PL, Metcalfe DD, O'Connor R, Muraro A, Rudman A, Schmitt C, Scherrer D, Simons FER, Thomas S, Wood JP, Decker WW (2006) Second symposium on the definition and management of anaphylaxis: summary report—second National Institute of allergy and infectious disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol 117:391–397
Sidhu N, Jones S, Perry T, Thompson T, Storm E, Melguizo Castro MS, Nick TG (2016) Evaluation of anaphylaxis management in a pediatric emergency department. Pediatr Emerg Care 32:508–513
Simons FER (2010) Anaphylaxis. J Allergy Clin Immunol 125:S161–S181
Sischerer SH, Simons FER (2017) Section on allergy and immunology. Epinephrine for first-aid management of anaphylaxis. Pediatrics 139:e20164006
Thomson H, Seith R, Craig S (2017) Inaccurate diagnosis of paediatric anaphylaxis in three Australian emergency departments. J Paediatr Child Health 53:698–704
Tiyyagura GK, Arnold L, Cone DC, Langhan M (2014) Pediatric anaphylaxis management in the prehospital setting. Prehosp Emerg Care 18:46–51
Walsh KE, Cutrona SL, Foy S, Baker MA, Forrow S, Shoaibi A, Pawloski PA, Conroy M, Fine AM, Nigrovic LE, Selvam N, Selvan MS, Cooper WO, Andrade S (2013) Validation of anaphylaxis in the Food and Drug Administration’s mini-sentinel. Pharmacoepidemiol Drug Saf 22:1205–1213
Wright CD, Longjohn M, Lieberman PL, Lieberman JA (2017) An analysis of anaphylaxis cases at a single pediatric emergency department during a 1-year period. Ann Allergy Asthma Immunol 118:461–464
Author information
Authors and Affiliations
Contributions
JCD, MSL, and GN conceived the study and designed the trial. JCD, JV, MSL, PM, AB, AC, and GV supervised data collection. GN provided statistical advice on study design and analyzed the data. JCD, MSL, and JV drafted the manuscript, and all authors contributed substantially to its revision. JCD takes responsibility for the paper as a whole.
Corresponding author
Ethics declarations
This study was approved by the Ethics Committee of the French Society of Pediatrics (Société Française de Pédiatrie, No. 2016_018_2) and the National Commission of Informatics and Liberty (Commission Nationale Informatique et Libertés, No. 2016-16).
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Additional information
Communicated by Nicole Ritz
Rights and permissions
About this article

Cite this article
Dubus, JC., Lê, MS., Vitte, J. et al. Use of epinephrine in emergency department depends on anaphylaxis severity in children. Eur J Pediatr 178, 69–75 (2019). https://doi.org/10.1007/s00431-018-3246-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-018-3246-3