
Abstract
Purpose
Respiratory support is the mainstay for the management of patients with pulmonary contusion following blunt chest trauma. In patients not requiring immediate intubation and ventilation, the optimal respiratory management strategy is not clear. This systematic review and meta-analysis aimed to determine the efficacy of non-invasive ventilation (NIV), as compared to traditional respiratory support strategies (i.e., high-flow facemask oxygen or pre-emptive intubation and ventilation), in adult patients with blunt chest trauma.
Methods
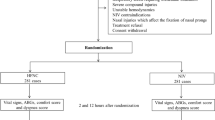
We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing NIV to traditional forms of respiratory support (i.e., facemask oxygen or intubation and ventilation) in an adult trauma population. For each eligible trial, we extracted the outcomes of all-cause mortality, length of intensive care unit (ICU) stay, length of hospital stay, and pneumonia.
Results
We identified 643 citations, selected 17 for full-text evaluation, and identified three eligible RCTs. Patients receiving NIV had a non-significant reduction in the risk of death (OR 0.55; 95 % CI 0.18–1.70; I 2 = 0 %), but significant reductions in length of ICU stay (mean difference −2.45 days; 95 % CI −4.27 to −0.63; I 2 = 66 %), length of hospital stay (mean difference −4.60 days; 95 % CI −8.81 to −0.39; I 2 = 85 %), and risk of pneumonia (OR 0.20; 95 % CI 0.09–0.47; I 2 = 0 %).
Conclusion
This meta-analysis suggests that NIV is superior to both high-flow facemask oxygen or pre-emptive intubation and ventilation in patients with blunt chest trauma who have no contraindication to NIV.





Similar content being viewed by others


References
Borman JB, et al. Unilateral flail chest is seldom a lethal injury. Emerg Med J. 2006;23(12):903–5.
Galan G, et al. Blunt chest injuries in 1696 patients. Eur J Cardiothorac Surg. 1992;6(6):284–7.
Richardson JD, Adams L, Flint LM. Selective management of flail chest and pulmonary contusion. Ann Surg. 1982;196(4):481–7.
Veysi VT, et al. Prevalence of chest trauma, associated injuries and mortality: a level I trauma centre experience. Int Orthop. 2009;33(5):1425–33.
Wanek S, Mayberry JC. Blunt thoracic trauma: flail chest, pulmonary contusion, and blast injury. Crit Care Clin. 2004;20(1):71–81.
Bastos R, Calhoon JH, Baisden CE. Flail chest and pulmonary contusion. Semin Thorac Cardiovasc Surg. 2008;20(1):39–45.
Nirula R, Mayberry JC. Rib fracture fixation: controversies and technical challenges. Am Surg. 2010;76(8):793–802.
Trinkle JK, et al. Management of flail chest without mechanical ventilation. Ann Thorac Surg. 1975;19(4):355–63.
Klopfenstein CE, Forster A, Suter PM. Pneumocephalus. A complication of continuous positive airway pressure after trauma. Chest. 1980;78(4):656–7.
Kaunitz VH. Flail chest. J Thoracic Cardiovasc Surg. 1981;82(3):463.
Linton DM, Potgieter PD. Conservative management of blunt chest trauma. S Afr Med J Suid-Afrikaanse Tydskrif Vir Geneeskunde. 1982;61(24):917–9.
Tranbaugh RF, Lewis FR. Respiratory insufficiency. Surg Clin North Am. 1982;62(1):121–32.
Hurst JM, DeHaven CB, Branson RD. Use of CPAP mask as the sole mode of ventilatory support in trauma patients with mild to moderate respiratory insufficiency. J Trauma-Injury Infect Crit Care. 1985;25(11):1065–8.
Potgieter PD, Rosenthal E, Benatar SR. Immediate and long-term survival in patients admitted to a respiratory ICU. Crit Care Med. 1985;13(10):798–802.
Bolliger CT, Van Eeden SF. Treatment of multiple rib fractures. Randomized controlled trial comparing ventilatory with nonventilatory management. Chest. 1990;97(4):943–8.
Walz M, Mollenhoff G, Muhr G. CPAP-augmented spontaneous respiration in thoracic trauma. An alternative to intubation. Unfallchirurg. 1998;101(7):527–36.
Beltrame F, et al. Noninvasive positive pressure ventilation in trauma patients with acute respiratory failure. Monaldi Arch Chest Dis. 1999;54(2):109–14.
Garfield MJ, Howard-Griffin RM. Non-invasive positive pressure ventilation for severe thoracic trauma. Br J Anaesth. 2000;85(5):788–90.
Wanek S, Mayberry JC. Blunt thoracic trauma: flail chest, pulmonary contusion, and blast injury. Crit Care Clin. 2004;20(1):71–81.
Balci AE, et al. Unilateral post-traumatic pulmonary contusion: findings of a review. Surg Today. 2005;35(3):205–10.
Gunduz M, et al. A comparative study of continuous positive airway pressure (CPAP) and intermittent positive pressure ventilation (IPPV) in patients with flail chest. Emerg Med J. 2005;22(5):325–9.
Xirouchaki N, et al. Noninvasive bilevel positive pressure ventilation in patients with blunt thoracic trauma. Respiration. 2005;72(5):517–22.
Trevisan CE, Vieira SR. Noninvasive mechanical ventilation may be useful in treating patients who fail weaning from invasive mechanical ventilation: a randomized clinical trial. Crit Care. 2008;12(2):R51.
Hernandez G, et al. Noninvasive ventilation reduces intubation in chest trauma-related hypoxemia: a randomized clinical trial. Chest. 2010;137(1):74–80.
Wigfield C et al. Oxygenation after pulmonary contusion in blunt thoracic trauma. Am J Respir Crit Care Med. Conference: American Thoracic Society International Conference, ATS, 2011. 183 (1 Meeting Abstracts).
Cohn SM, Dubose JJ. Pulmonary contusion: an update on recent advances in clinical management. World J Surg. 2010;34(8):1959–70.
Clemedson CJ. Blast injury. Physiol Rev. 1956;36(3):336–54.
Miller PR, et al. Acute respiratory distress syndrome in blunt trauma: identification of independent risk factors. Am Surg. 2002;68(10):845–50 discussion 850–1.
Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Acknowledgments
Dr Rodseth is supported by a CIHR Scholarship (the Canada-HOPE Scholarship), Ottawa, Canada; the College of Medicine of South Africa (the Phyllis Kocker/Bradlow Award), Cape Town, South Africa; and the University of KwaZulu-Natal (competitive research grant), Durban, South Africa. Dr Biccard is supported by a National Research Foundation (NRF) grant and the University of KwaZulu-Natal (competitive research grant).
Conflict of interest
Dr’s Roberts, Skinner, Biccard and Rodseth declare that they have no conflict of interest.
Compliance with Ethics Guidelines
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Appendix 1: Search strategy and databases
Appendix 1: Search strategy and databases
Database searches were conducted on 18 September 2012 using the OvidSP search engine (Ovid Technologies, Inc., New York, NY 2009) for the following databases:
-
1.
EMBASE 1979–2012 September 17
-
2.
OVID Health Star (1966–August 2012)
-
3.
Ovid MEDLINE(R) In-Process and Other Non-Indexed Citations and OVID MEDLINE(R) 1946 to present
-
4.
Cochrane Central Register of Controlled Trials (September 2012)
-
5.
Cochrane Database of Systematic Reviews (September 2012)
The MESH search terms used in Medline, OVID Health Star, and the Cochrane data bases were (1) Positive-Pressure Respiration.mp; and (2) Wounds and Injuries.mp. The EMBASE search terms used were: (1) Thorax injury.mp; and (2) artificial ventilation.mp.
Rights and permissions
About this article
Cite this article
Roberts, S., Skinner, D., Biccard, B. et al. The role of non-invasive ventilation in blunt chest trauma: systematic review and meta-analysis. Eur J Trauma Emerg Surg 40, 553–559 (2014). https://doi.org/10.1007/s00068-013-0370-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-013-0370-7