
Abstract
The aim of this study was to determine if dimensions and sub-categories of a previously-tested obtrusiveness framework were represented in interviews conducted with community-dwelling older adults at three- and six-month study visits during an in-home sensor study. Secondary analysis of interviews was performed using a codebook based on an obtrusiveness framework. Eight community-dwelling older adults aged 79–86 participated in 15 interviews. One participant died between the three- and six-month interviews. Some elements of the obtrusiveness framework were present at three months but not at six months, indicating that perceptions of obtrusiveness of in-home sensors may decline over time. Findings highlight the importance of privacy issues and perceived usefulness for sensor technology use and adoption. There is a need to develop an obtrusiveness assessment instrument that enables nuanced measurements based on specific contexts and types of technologies.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
1.1 Aging and Technology
An increase in the worldwide population of older adults is driving the need for innovative solutions to help older adults maintain independence at home and foster health. Smart home technologies, defined as sensing technologies embedded in the residential infrastructure to facilitate passive monitoring, have the potential to enable lasting independence. One potential application of smart home technologies to foster maximal health of older adults is through collection of information about activity levels in the home to support augmented cognition. This could enable older adults to monitor their own activity levels, leading to behavior change and more efficient self-management of health, or alert care providers and family members about changes in patterns that could indicate functional decline.
Technology is increasingly used to help older adults stay independent and connected to their health care providers [1]. Technology acceptance is an important factor in technology adoption and use [2]. Therefore, there is a need for research to identify what features and types of home monitoring technologies that are acceptable to older adults [3]. Over 93 % of older adults in the United States live independently in community settings [4] but not all people age the same way [5], or have the same views about the acceptability of technology [6] and health information sources [7]. Thus, determining the views of community-dwelling older adults regarding in-home sensors is important if these technologies are to be designed appropriately for different types of people and play a role in everyday health maintenance.
1.2 Obtrusiveness
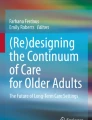
Obtrusiveness, defined as “a summary evaluation by the user based on characteristics or effects associated with the technology that are perceived as undesirable and physically and/or psychologically prominent” [8] (p. 430), is a factor in technology acceptance. While there is a recognized need to understand older adults’ views about obtrusiveness of smart home technologies and how these views change over time, validated instruments that measure obtrusiveness of technology do not yet exist [9]. Hensel et al. developed a conceptual framework that describes eight broad dimensions of obtrusiveness for smart home technologies [8] (see Fig. 1).

Obtrusiveness framework with dimensions and subcategories based on Hensel et al. [8]
Courtney et al. validated this framework [10] with older adults at a continuing care retirement community (CCRC) [11] and two residential care communities [12]. The framework has subsequently been used to engage older adults regarding their perceptions of technology obtrusiveness to aid the creation of design guidelines for smart home technologies [13] and to determine the effect of distinct sensing approaches on older adults’ perceptions of technologies [14]. However, the views of community-dwelling older adults regarding the obtrusiveness of smart homes technologies installed in their homes remain largely unexplored, and individual studies do not evaluate changes in older adults’ perceptions of obtrusiveness over long periods of time. Therefore, the aim of this study was to determine if the dimensions and sub-categories of an obtrusiveness framework were represented in technology acceptance interviews with community-dwelling older adults through secondary analysis of interview data collected at three- and six-month study visits during an in-home sensor study.
2 Methods
This study was a secondary analysis of interviews conducted as part of a six-month feasibility study of smart home technologies [15] installed in the homes of community-dwelling older adults in the Pacific Northwest region of the United States. The study setting was an independent retirement community in the Pacific Northwest region of the United States [15]. All residents are independent living. The community consists of a mix of 1-, 2- and 3-bedroom apartments with communal living spaces such as a gym, patio and library available to residents. All residences are provided with Internet access.
A convenience sample of participants was recruited through a presentation at the study setting and through the use of snowball sampling procedures. Inclusion criteria were to be a resident within the participating retirement community 65 years of age or older and able to speak and understand written English. Written informed consent was obtained from participants prior to study procedures. All study procedures were approved by the Institutional Review Board of the University of Washington.
All participants were administered a battery of standardized instruments that measured a variety of physical, psychosocial, and cognitive parameters at baseline and 6-month data collection visits. A full description of the study protocol, instruments administered and data collection schedule for each instrument is available in the primary study publication [15]. All participants were found to have normal cognition after screening for cognitive impairment using the Mini-Cog cognitive screening tool [16]. At the three- and six-month visits, semi-structured interviews to solicit participants’ attitudes toward in-home sensor technologies were conducted and recorded with a digital audio recorder. Interview questions related to obtrusiveness, usefulness and acceptability of technology. The full interview guide is available in the primary study publication [15].
2.1 Sensor System
The smart home technologies used in this study consisted of in-home sensor systems that used commercially available passive infrared motion sensors, a gateway and a secure web-based interface for system administration and sensor data visualization. Sensor data were transmitted wirelessly to the gateway and then transferred over the Internet to a remote server. Sensors were installed in the living spaces of each participant including bedrooms, living rooms, kitchens, dining rooms and bathrooms. The number of sensors installed in each residence varied based on the size and layout of the residence. Additional details about the sensor system and installations are available in the primary study publication [15].
Sensor systems were installed in the home of each participant during enrollment. The function of the sensor system was described to participants during recruiting efforts and enrollment procedures. Specifically, participants were informed that the sensor system did not collect video data or personally identifiable information beyond activity levels. Specific information regarding the obtrusiveness framework was not provided to study participants.
2.2 Data Analysis
A secondary analysis of technology acceptance interviews from the main study was performed using a theory-driven coding approach [17]. The approach was theory-driven in that it relied on a codebook based on the obtrusiveness framework [8, 10]. A version of this codebook was previously used to analyze qualitative data obtained in studies of older adults at a continuing care retirement community and two residential care communities [10]. The codebook was obtained from one of the developers of the framework.
Interviews were transcribed verbatim. The coding team consisted of the study leader and three research team members. The study leader had five years of extensive qualitative data collection and analysis experience. One of the study PIs provided guidance and oversight regarding application of the codebook. This PI originally trained the study leader in qualitative data analysis and was one of the developers of the obtrusiveness framework and codebook. The three research team members were doctoral students with qualitative analysis experience obtained through graduate course work and from projects within the research group.
The three research team members independently coded transcripts from 3 month (n = 8) and 6 month interviews (n = 7). The study leader, acting as a fourth coder, independently analyzed sets of coded transcripts and noted disagreements between coders. Disagreements were reconciled through discussion during in-person meetings of all coders until consensus was reached about application of codes.
Our total data set consisted of 15 interviews. Within the focus and constraints of our study, we believe that data saturation was reached. O’Reilly and Parker note that data saturation is a contentious issue with complexities such that the concept may not plausibly transfer in the same way across qualitative approaches [18]. For data-driven qualitative analysis, Guest et al. showed that 94 % of all high-frequency codes were identified within the first six interviews and 97 % within the first 12 interviews [19]. For theory-based studies, Francis et al. recommend specifying an initial sample size and an additional number of interviews as a stopping criterion, demonstrating the approach with retrospective analysis of 10 and 3 interviews [20]. Given our sample size and approach, our study functionally satisfies the recommendations of both Guest et al. [19] and Francis et al. [20].
3 Results
Eight participants ranging in age from 79 to 86 years (mean age 83 ± 2.2) enrolled in the study. All participants were Caucasian and 75 % had completed graduate school. One participant died between the three- and six-month study visits. Table 1 shows the dimensions and subcategories of the obtrusiveness framework that were represented in three- and six- month interviews. Check marks represent instances where participant responses indicated the dimension or subcategory was a concern.
3.1 Physical Dimension
Overall, participants found the smart home technologies installed in their homes to be non-obtrusive, as illustrated by the following quote. “I don’t even remember they’re there. Most of the time, I don’t even think about it. It wouldn’t occupy a tenth of 1 % of my time. I just come in and live in here” (participant at 3 months). The only subcategory represented in this dimension was “Aesthetic incongruence or excessive noise”. Referring to the gateway hardware, one participant commented: “I wanted to push this thing out of the way so it wouldn’t look so obvious” (at 3 months). In addition, she stated that visitors frequently asked about the sensor system: “The only time I think about it is when someone says, and this happens fairly often, ‘What the heck are those supposed to be doing?’” (at 3 months) but later observed: “I don’t think anyone’s said anything about them for a couple of months” (at 6 months). Another participant did not find the system obtrusive but noted that others might: “If you are someone who insists on décor then it might be bothersome” (at 6 months).
3.2 Usability Dimension
The technology used in this study consisted solely of sensors and gateways that were installed by members of the research team and were at no point operated by the residents. As such usability issues resulting from a potential interaction with the system were not applicable to this study.
3.3 Privacy Dimension
There were few instances where perceptions pertaining to the subcategory “Invasion of personal information” emerged in participants’ responses. Participants discussed their assumptions that personal activity data would be de-identified and secured: “It’s fine. Nobody knows who I am, what I do” (participant at 3 months) and “I just trust the people that would be gathering this information that they keep it” (participant at 3 months). Regarding the “Violation of personal space” subcategory, one participant reported having to renegotiate his understanding of how the system worked when he noticed a sensor in the bathroom: “Every once in a while I think that: ‘No, that thing is not taking pictures’” (at 3 months). Later, he stated: “Early on I noticed them when I went in the bathroom, and then it would dawn on me: ‘No, that’s not a camera.’ So it was just reminding myself what it really was and then I forgot all about it” (at 6 months).
3.4 Function Dimension
Issues related to the “Malfunction or unreliable performance” and “Inaccurate measurement” subcategories were represented as doubts about unproven technology in both three- and six-month interviews. For example, one participant was concerned that measurements from the sensor in her laundry room might be inaccurately mistaken for bathroom sensor measurements. Her comment was: “Do they remember that I said this is my laundry? This is where I do the washing and the ironing. So I may be in there ironing and listening to the radio for a couple of hours or maybe a ten minute session if I’m just pressing something. But you know, I think: ‘So what difference does it make? But I want them to know I’m not ill. (laughs) I’m healthy and hearty at the moment” (at 6 months).
For the “Perceived lack of usefulness” subcategory, coded responses about the usefulness of activity data from smart home technologies were mixed. One view was that health care providers should have as much information as possible: “I think they should know as much as they can know about because otherwise it’s hard for them to treat us” (participant at 3 months). However, this same participant did not see the usefulness of smart home technologies for herself. Another participant commented: “I would like to see the results of the finished project but I have no idea whether it would have any usefulness to me” (at 3 months). Another participant felt that personal activity data could be useful in interactions with health care providers when discussing issues related to chronic pain: “I tell him: ‘I have sleep interruptions.’ ‘How do you know that?’ ‘Well, I say, I’ve got data” (at 3 months).
3.5 Human Dimension
“Lack of human response in emergencies” was not seen as a concern. To the contrary, technology was seen as potentially supportive of human response in an emergency. The following quote exhibits a preventive mindset: “If I get to the point where I am falling, I want a sensor. I don’t want to lay here for two days without anybody knowing there is something wrong with me” (participant at 6 months). This participant acknowledged the need for technology to alert people to respond in the event of an emergency. Likewise, the same held true for the “Detrimental to relationships” subcategory; several participants reported that they volunteered information about the study to visiting family members and friends.
3.6 Self-concept Dimension
Subcategories in this dimension were not represented.
3.7 Routine Dimension
Issues related to the “Interference with daily activities” and “Acquisition of new rituals” subcategories were raised by one participant. His concern related to having to sign in and out of the building so the system would not raise alarms due to lack of motion in his residence. In discussion of schedule coordination with activity data, he commented: “That would require that I somehow notify the system that I’m gonna be gone, and you know, that would be the same as my signing out. I don’t do it and I wouldn’t be likely to do it” (at 3 months).
3.8 Sustainability Dimension
The “Affordability” or “Concern about future needs and abilities” (as they relate to participant capacity to operate or use the technology) subcategories were not represented. This absence may be due to participant thinking about the need (or lack thereof) for smart home technologies. For instance, when asked about sharing personal activity data, one participant expressed a lack of concern about need for technology and an overall comfort with the stability of her physical abilities: “I don’t think so at the moment. Not unless my behavior, my physical condition, changes considerably. But I’m pretty much the way I’ve been for the past I don’t know how many years” (at 3 months). In addition, the affordability issue may not have been raised because the technology in the study was installed free of charge.
4 Conclusion
This study explored the dimensions of an obtrusiveness framework with community-dwelling older adults living in an independent retirement community whereas prior research did so with residents of a CCRC and two residential care communities [10]. A particular strength of this study is that our protocol was longitudinal in nature, giving us the opportunity to compare differences in presence of elements of the obtrusiveness framework from participant interviews at three and six months. As such, this study contributes to knowledge about aging and technology regarding obtrusiveness and its dimensions.
Participants expressed minor concerns in the Physical and Routine dimensions during 3 month interviews. Issues regarding aesthetic incongruence and changes in routine raised during 3 month interviews resolved themselves for study participants by the 6 month visit. These results suggest that some older adult concerns about technologies installed their homes diminish over time. This is consistent with other studies of home based technologies that indicate that home care patients had a more positive attitude towards the technology as time passed [21].
Noting potential limitations when comparing different interview protocols and study aims we contrast our results to prior research that tested the obtrusiveness framework with participants from different settings [10]. The Privacy (Invasion of personal information and Violation of personal space of the home) and Function (Perception of lack of usefulness) dimensions were represented in data collected from community-dwelling older adults in this study and in prior studies with residents of residential care facilities and CCRCs [10]. This finding confirms the acknowledged importance of privacy issues and perceived usefulness concerning health-related technology use and adoption. Conversely, whereas the dimensions of Human Interaction (Lack of human response in emergencies), Self-Concept (Symbol of loss of independence, Cause of embarrassment or stigma) and Sustainability (Concern about affordability) were present in interviews of residents of residential care facilities and CCRCs [10], these dimensions were absent in our interviews of community-dwelling older adults. This finding suggests that independent living community-dwelling older adults may not have concerns in these areas because of differences in circumstances related to health or living situation. An important area for future work would be to confirm this initial understanding by comparing older adults’ perceptions across settings in a single study. This would also assist in the development of instruments to measure obtrusiveness.
Limitations of this study include a small sample size with a racially homogenous sample with a higher level of educational attainment than the general US population of adults 65 years of age and older. Thus, the findings may not generalize to larger populations of older adults within or external to the US. However in spite of these limitations, the study provides insight into older adults’ perceptions of obtrusiveness in a longitudinal study of smart home technologies, providing new understanding in an underexplored area.
Deployments of smart home technologies will vary based on context and the target population who use them because people age differently and have different needs. The technologies deployed in this study included commercially available sensors that have been deployed in other smart home studies [22]. Since more than 93 % of older adults in the United States live independently in community settings [4], one of our study aims was to determine technology perceptions for healthy community-dwelling older adults to inform future preventive interventions.
While the obtrusiveness framework used in this study should be further validated, its dimensions appear to hold for older adults in a range of different settings. The implications are that the construct of the framework seems valid but the prevalence of dimensions varies by context. This idea suggests the need to develop an instrument that affords nuanced, context-based measurements of the obtrusiveness of smart home technologies. Thus, an instrument to measure obtrusiveness of smart home technologies may require modification based on specific contexts and technologies. Therefore, future research to develop a validated instrument should focus on the type and frequency of concerns as they relate to the dimension of the obtrusiveness framework when it is administered across settings and to individuals across a range of older adult’s health status.
References
Reeder, B., Chung, J., Stevens-Lapsley, J.: Current telerehabilitation research with older adults at home: an integrative review. J. Gerontological Nurs. (In press)
Davis, F.D.: Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 13, 319–340 (1989)
Kang, H.G., Mahoney, D.F., Hoenig, H., Hirth, V.A., Bonato, P., Hajjar, I., Lipsitz, L.A.: In situ monitoring of health in older adults: technologies and issues. J. Am. Geriatr. Soc. 58, 1579–1586 (2010)
United States Federal Interagency Forum on Aging-Related Statistics: Older Americans 2010: Key Indicators of Well-Being. Government Printing Office, Washington, DC (2010)
Zaslavsky, O., Cochrane, B.B., Herting, J.R., Thompson, H.J., Woods, N.F., Lacroix, A.: Application of person-centered analytic methodology in longitudinal research: exemplars from the Women’s Health Initiative Clinical Trial data. Res. Nurs. Health 37, 53–64 (2014)
Caine, K.E., Fisk, A.D., Rogers, W.A.: Benefits and privacy concerns of a home equipped with a visual sensing system: A perspective from older adults. In: Proceedings of the Human Factors and Ergonomics Society Annual Meeting, vol. 50, pp. 180–184. Sage Publications (2006)
Le, T., Chaudhuri, S., White, C., Thompson, H., Demiris, G.: Trust in health information sources differs between young/middle and oldest old. Am. J. Health Promot. AJHP 28, 239–241 (2014)
Hensel, B.K., Demiris, G., Courtney, K.L.: Defining obtrusiveness in home telehealth technologies a conceptual framework. J. Am. Med. Inf. Assoc. 13, 428–431 (2006)
Daniel, K.M., Cason, C.L., Ferrell, S.: Emerging technologies to enhance the safety of older people in their homes. Geriatr. Nurs. 30, 384–389 (2009)
Courtney, K.L., Demiris, G., Hensel, B.K.: Obtrusiveness of information-based assistive technologies as perceived by older adults in residential care facilities: A secondary analysis. Med. Inf. Internet Med. 32, 241–249 (2007)
Demiris, G., Rantz, M.J., Aud, M.A., Marek, K.D., Tyrer, H.W., Skubic, M., Hussam, A.A.: Older adults’ attitudes towards and perceptions of ‘smart home’ technologies: a pilot study. Inf. Health Soc. Care 29, 87–94 (2004)
Courtney, K.L.: Privacy and senior willingness to adopt smart home information technology in residential care facilities. Methods Inf. Med. 47, 76–81 (2008)
Meulendijk, M., Van De Wijngaert, L., Brinkkemper, S., Leenstra, H.: Am I in good care? Developing design principles for ambient intelligent domotics for elderly. Inf. Health Soc. Care 36, 75–88 (2011)
Demiris, G.: Privacy and social implications of distinct sensing approaches to implementing smart homes for older adults. Engineering in Medicine and Biology Society, 2009, EMBC 2009, Annual International Conference of the IEEE, pp. 4311–4314. IEEE (2009)
Reeder, B., Chung, J., Lazar, A., Joe, J., Demiris, G., Thompson, H.J.: Testing a theory-based mobility monitoring protocol using in-home sensors: a feasibility study. Res. Gerontol Nurs. 6, 253–263 (2013)
Borson, S., Scanlan, J., Brush, M., Vitaliano, P., Dokmak, A.: The mini-cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int. J. Geriatr. Psychiatry 15, 1021–1027 (2000)
Boyatzis, R.E.: Transforming qualitative information: thematic analysis and code development. Sage Publications, Thousand Oaks (1998)
O’Reilly, M., Parker, N.: ‘Unsatisfactory Saturation’: a critical exploration of the notion of saturated sample sizes in qualitative research. Qual. Res. 13, 190–197 (2013)
Guest, G., Bunce, A., Johnson, L.: How many interviews are enough? Field Methods 18, 59–82 (2006)
Francis, J.J., Johnston, M., Robertson, C., Glidewell, L., Entwistle, V., Eccles, M.P., Grimshaw, J.M.: What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol. Health 25, 1229–1245 (2010)
Demiris, G., Speedie, S.M., Finkelstein, S.: Change of patients’ perceptions of TeleHomeCare. Telemed. J. e-Health 7, 241–248 (2001)
Reeder, B., Meyer, E., Lazar, A., Chaudhuri, S., Thompson, H.J., Demiris, G.: Framing the evidence for health smart homes and home-based consumer health technologies as a public health intervention for independent aging: A systematic review. Int. J. Med. Inf. 82, 565–579 (2013)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this paper
Cite this paper
Reeder, B., Chung, J., Joe, J., Lazar, A., Thompson, H.J., Demiris, G. (2016). Understanding Older Adults’ Perceptions of In-Home Sensors Using an Obtrusiveness Framework. In: Schmorrow, D., Fidopiastis, C. (eds) Foundations of Augmented Cognition: Neuroergonomics and Operational Neuroscience. AC 2016. Lecture Notes in Computer Science(), vol 9744. Springer, Cham. https://doi.org/10.1007/978-3-319-39952-2_34
Download citation
DOI: https://doi.org/10.1007/978-3-319-39952-2_34
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-39951-5
Online ISBN: 978-3-319-39952-2
eBook Packages: Computer ScienceComputer Science (R0)