World Journal of Emergency Medicine ›› 2013, Vol. 4 ›› Issue (4): 266-272.doi: 10.5847/wjem.j.issn.1920-8642.2013.04.004
• Original Articles • Previous Articles Next Articles
Xu-rui Luo, Hui-li Zhang, Geng-jin Chen, Wen-shu Ding, Liang Huang( )
)
Received:2013-03-10
Accepted:2013-07-20
Online:2013-12-15
Published:2013-12-15
Contact:
Liang Huang
E-mail:huangliang6312@sina.com
Xu-rui Luo, Hui-li Zhang, Geng-jin Chen, Wen-shu Ding, Liang Huang. Active compression-decompression cardiopulmonary resuscitation (CPR) versus standard CPR for cardiac arrest patients: a meta-analysis[J]. World Journal of Emergency Medicine, 2013, 4(4): 266-272.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.issn.1920-8642.2013.04.004
Figure 1.
Searching strategy.
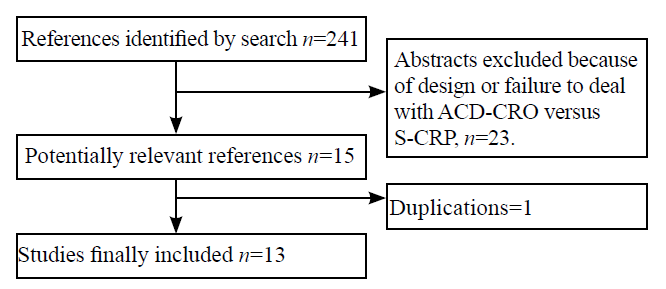
Table 1
General information about included studies
| Author | Patients (T/C) | Age | Treatment (T/C) | Outcome | Circumstances where patients confronted CA | Country |
|---|---|---|---|---|---|---|
| 2009 Chen SP | 109/109 | ≥18 | T: ACD-CPR C: standard CRP | ROSC Survival rate at 24 hours | Out-of-hospital | China |
| 2003 He Q | 46/46 | ≥18 | T: ACD-CPR C: standard CRP | ROSC Survival rate to hospital admission | In-hospital | China |
| 1999 Baubin M | 33/15 | ≥18 | T1: ACD-CPR C: standard CRP | Ventricular fibrillation Complications of CPR (sternal fractures) | Out-of-hospital | Australia |
| 1999 Plaisance P | 373/377 | ≥18 | T: ACD-CPR C: standard CRP | Hospital discharge rate without neurologic impairment One-year survival rate | Out-of-hospital | France |
| 1997 Mauer D | - | ≥18 | T: ACD-CPR C: standard CRP | Survival rate Neurological outcome Complications of CPR | Out-of-hospital | Germany |
| 1997 Plaisance P | 254/258 | ≥18 | T: ACD-CPR C: standard CRP | ROSC Survival rate at 1 hour, 24 hours, and 1 month Survival rate to hospital discharge without neurological impairment Neurological outcome Complications of CPR | Out-of-hospital | France |
| 1996 Luiz T | 26/30 | ≥18 | T: ACD-CPR C: standard CRP | ROSC Mean carbon dioxide content | Out-of-hospital | Germany |
| 1996 Mauer D | 106/114 | ≥18 | T: ACD-CPR C: standard CRP | ROSC Survival rate to hospital admission Survival rate to hospital discharge Neurological outcome (CPC and OPC) Complications of CPR | Out-of-hospital | Germany |
| 1996 Stiell IG | 405/368 | ≥18 | T: ACD-CPR C: standard CRP | Survival rate to hospital discharge Neurological outcome | In-hospital | Canada |
| 1996 Stiell IG | 501/510 | ≥18 | T: ACD-CPR C: standard CRP | Survival rate to hospital discharge Neurological outcome | Out-of-hospital | Canada |
| 1994 Ellinger K | 26/30 | ≥18 | T: ACD-CPR C: standard CRP | ROSC Survival rate to hospital discharge Complications of CPR | Out-of-hospital | Germany |
| 1994 Tucker KJ | 25/28 | ≥18 | T: ACD-CPR C: standard CRP | ROSC Survival rate at 24 hours Surivival rate to hospital discharge | In-hospital | USA |
| 1993 Cohen TJ | 29/33 | ≥18 | T: ACD-CPR C: standard CRP | Rages of initial resuscitation Survival rate at 24 hours Survival rate to hospital discharge Neurological outcome | In-hospital | USA |
Table 2
Quality of the included studies
| Author | Random method | Blind allocation | Concealed allocation | Exit/Out of research | Comparability of base line | Jadad score |
|---|---|---|---|---|---|---|
| 2009 Chen SP | Not described | No | No | No | Yes | 1 |
| 2003 He Q | Not described | No | No | No | Yes | 1 |
| 1999 Baubin M | Not described | No | No | No | Yes | 1 |
| 1999 Plaisance P | Assigned on an even or odd day of the month | No | Yes | No | Yes | 2 |
| 1999 Sklgvoll E | A random number tag | No | Yes | No | Yes | 3 |
| 1997 Mauer D | Not described | No | No | No | Yes | 1 |
| 1997 Plaisance P | Assigned on an even or odd day of the month | No | No | No | Yes | 1 |
| 1996 Luiz T | Not described | No | No | No | Yes | 1 |
| 1996 Mauer D | Not described | No | No | No | Yes | 1 |
| 1996 Stiell IG | Allocation by using a sealed container | Yes | Yes | No | Yes | 5 |
| 1994 Ellinger K | Not described | No | No | No | Yes | 1 |
| 1994 Tucker KJ | Not described | No | No | No | Yes | 1 |
| 1993 Cohen TJ | Assigned on medical-record numbers | No | Yes | No | Yes | 2 |
| 1993 Pell AC | Not described | No | No | No | Yes | 1 |

Figure 2.
Comparison of ROSC rate between the ACD-CPR group and the S-CPR group.
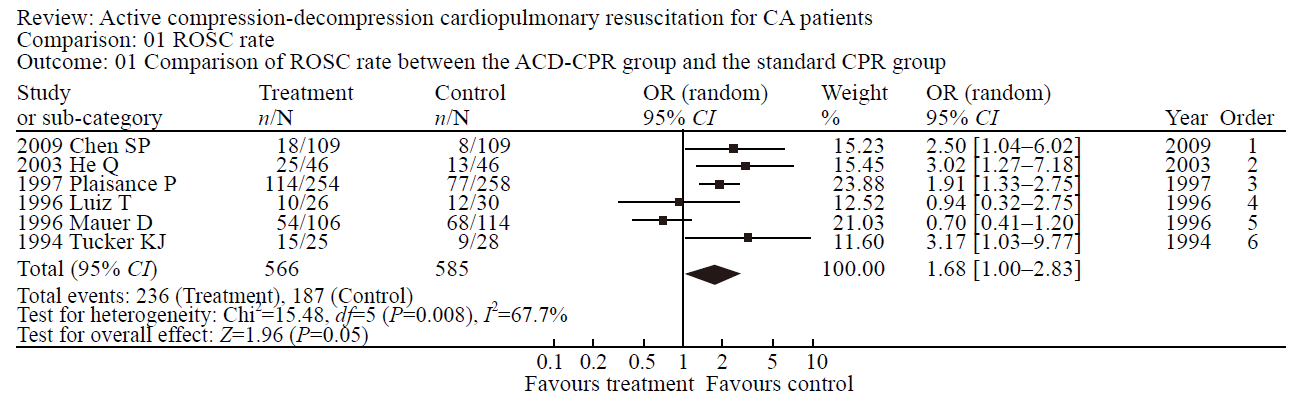
Figure 3.
Comparison of hospital admission rate between the ACD-CPR group and the S-CPR group.
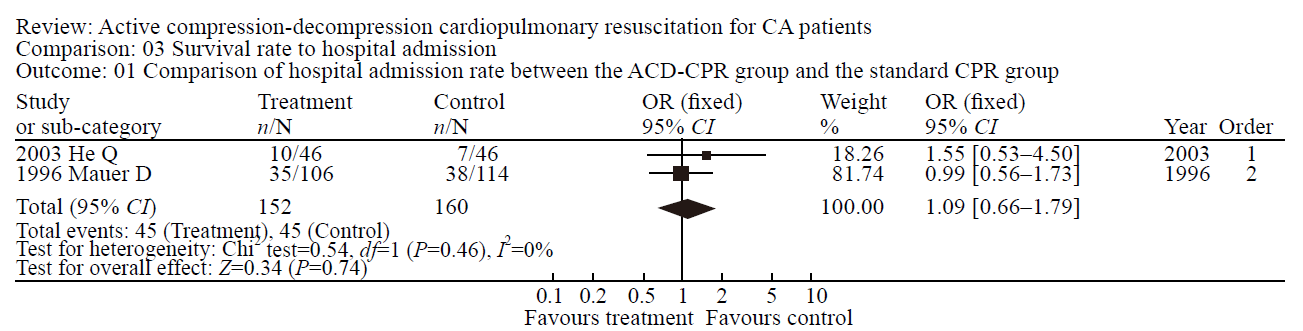
Figure 4.
Survival rate comparison at 24 hours between the ACD-CPR group and the S-CPR group.

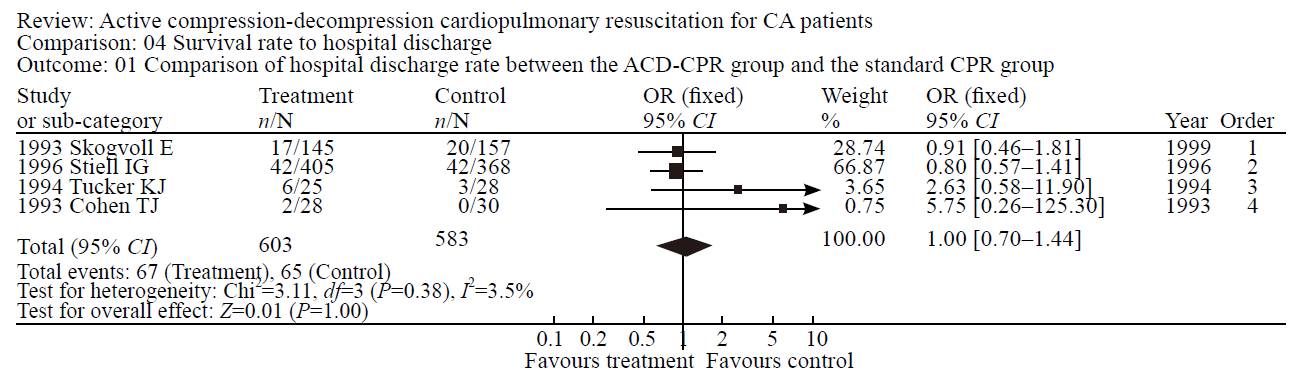
Figure 5.
Hospital discharge rate comparison between the ACD-CPR group and the S-CPR group.
| 1 |
Zheng ZJ, Croft JB, Giles WH, Mensah GA. Sudden cardiac death in the United States, 1989 to 1998. Circulation 2001; 104:2158-2163.
doi: 10.1161/hc4301.098254 pmid: 11684624 |
| 2 | Neumar RW, Otto CW, Link MS, Kronick SL, Shuster M, Callaway CW, et al. Adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation 2010; 122:729-767. |
| 3 |
Jiang L, Zhang JS. Mechanical cardiopulmonary resuscitation for patients with cardiac arrest. World J Emerg Med 2011; 2:165-168.
pmid: 25215003 |
| 4 |
von Planta I, Wagner O, von Planta M, Ritz R. Determinants of survival after rodent cardiac arrest: implications for therapy with adrenergic agents. Int J Cardiol 1993; 38:235-245.
pmid: 8096498 |
| 5 |
Deakin CD, Nolan JP, Soar J, Sunde K, Koster RW, Smith GB, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 4. Adult advanced life support. Resuscitation 2010; 81:1305-1352.
doi: 10.1016/j.resuscitation.2010.08.017 pmid: 20956049 |
| 6 |
Aufderheide TP, Frascone RJ, Wayne MA, Mahoney BD, Swor RA, Domeier RM, et al. Standard cardiopulmonary resuscitation versus active compression-decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out-of-hospital cardiac arrest: a randomized trial. Lancet 2011; 377:301-311.
pmid: 21251705 |
| 7 |
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials:is blinding necessary? Control Clin Trials 1996; 17:1-12.
doi: 10.1016/0197-2456(95)00134-4 pmid: 8721797 |
| 8 | Egger M, Smith GD, Douglas G. Systematic reviews in health care: meta-analysis in context. BMJ Books 2001; 2:3-475. |
| 9 |
Higgins JP, Thompson SG, Deek JJ, Altman DG. Measuring inconsistency in meta-analyses. Br Med J 2003; 327:557-560.
doi: 10.1136/bmj.327.7414.557 |
| 10 |
Higgins J, Thompson S, Deeks J, Altman D. Statistical heterogeneity in systematic reviews of clinical trials: a critical appraisal of guidelines and practice. J Health Serv Res Policy 2002; 7:51-61.
pmid: 11822262 |
| 11 |
Tang J, Liu JL. Misleading funnel plot for detection of bias in meta-analysis. J Clin Epidemiol 2000; 53:477-484.
doi: 10.1016/s0895-4356(99)00204-8 pmid: 10812319 |
| 12 | Chen SP. Curative effects of the heart pump in 109 pre-hospital cardiopulmonary resuscitation patients for cardiopulmonary resuscitation. Chin Crit 2009; 21:378. |
| 13 |
Kulstad EB, Courtney DM, Waller D. Induction of therapeutic hypothermia via the esophagus: a proof of concept study. World J Emerg Med 2012; 3:118-122.
pmid: 25215049 |
| 14 |
Baubin M, Sumann G, Rabl W, Eibl G, Wenzel V, Mair P. Increased frequency of thorax injuries with ACD-CPR. Resuscitation 1999; 41:33-38.
doi: 10.1016/s0300-9572(99)00033-7 pmid: 10459590 |
| 15 |
Plaisance P, Lurie KG, Vicaut E, Adnet F, Petit JL, Epain D, et al. A comparison of standard cardiopulmonary resuscitation and active compression-decompression resuscitation for out-of-hospital cardiac arrest. French Active Compression-Decompression Cardiopulmonary Resuscitation Study Group. N Engl J Med 1999; 341:569-575.
pmid: 10451462 |
| 16 |
Skogvoll E, Wik L. Active compression-decompression cardiopulmonary resuscitation: a population-based, prospective randomised clinical trial in out-of-hospital cardiac arrest. Resuscitation 1999; 42:163-172.
doi: 10.1016/s0300-9572(99)00086-6 pmid: 10625156 |
| 17 | Mauer D, Schneider T, Dick W, Elich D, Mauer M. Active compression-decompression resuscitation. Improved survival rate in an emergency medicine system with emergency physician assistance? Med Klin (Munich) 1997; 92:381-388. |
| 18 |
Plaisance P, Adnet F, Vicaut E, Hennequin B, Magne P, Prudhomme C, et al. Benefit of active compression-decompression cardiopulmonary resuscitation as a prehospital advanced cardiac life support. A randomized multicenter study. Circulation 1997; 95:955-961.
doi: 10.1161/01.cir.95.4.955 pmid: 9054757 |
| 19 |
Luiz T, Ellinger K, Denz C. Active compression-decompression cardiopulmonary resuscitation does not improve survival in patients with prehospital cardiac arrest in a physician-manned emergency medical system. Cardiothorac Vasc Anesth 1996; 10:178-186.
doi: 10.1016/S1053-0770(96)80234-5 |
| 20 |
Mauer D, Schneider T, Dick W, Withelm A, Elich D, Mauer M. Active compression-decompression resuscitation: a prospective, randomized study in a two-tiered EMS system with physicians in the field. Resuscitation 1996; 33:125-134.
doi: 10.1016/s0300-9572(96)01006-4 pmid: 9025128 |
| 21 |
Stiell IG, Hébert PC, Wells GA, Laupacis A, Vandemheen K, Dreyer JF, et al. The Ontario trial of active compression-decompression cardiopulmonary resuscitation for in-hospital and prehospital cardiac arrest. JAMA 1996; 275:1417-1423.
pmid: 8618367 |
| 22 |
Ellinger K, Luiz T, Denz C, van Ackern K. Randomized use of an active compression-decompression technique within the scope of preclinical resuscitation. Anasthesiol Intensivmed Notfallmed Schmerzther 1994; 29:492-500.
doi: 10.1055/s-2007-996790 pmid: 7841276 |
| 23 |
Tucker KJ, Galli F, Savitt MA, Kahsai D, Bresnahan L, Redberg RF. Active compression-decompression resuscitation: effect on resuscitation success after in-hospital cardiac arrest. J Am Coll Cardiol 1994; 24:201-209.
pmid: 8006266 |
| 24 |
Reynolds JC, Salcido DD, Menegazzi JJ. Correlation between coronary perfusion pressure and quantitative ECG waveform measures during resuscitation of prolonged ventricular fibrillation. Resuscitation 2012; 83:1497-1502.
pmid: 22562057 |
| 25 |
Wang HC, Chiang WC, Chen SY. Video recording and time motion analyses of manual versus mechanical cardiopulmonary resuscitation during ambulance transport. Resuscitation 2007; 74:453-460.
pmid: 17386966 |
| 26 |
Eisenberg MS, Cummins RO, Damon S, Larsen MP, Hearne TR. Survival rates from out-of-hospital cardiac arrest: recommendations for uniform definitions and data to report. Ann Emerg Med 1990; 19:1249-1259.
doi: 10.1016/s0196-0644(05)82283-8 pmid: 2240720 |
| 27 |
Shultz JJ, Coffeen P, Sweeney M, Detloff B, Kehler C, Pineda E, et al. Evaluation of standard and active compression-decompression CPR in an acute human model of ventricular fibrillation. Circulation 1994; 89:684-693.
pmid: 8313556 |
| 28 |
Orliaguet GA, Carli PA, Rozenberg A, Janniere D, Sauval P, Delpech P. End-tidal carbon dioxide during out-of-hospital cardiac arrest resuscitation: comparison of active compression-decompression and standard CPR. Ann Emerg Med 1995; 25:48-51.
doi: 10.1016/s0196-0644(95)70354-3 pmid: 7802369 |
| 29 |
Guly UM, Mitchell RG, Cook R, Steedman DJ, Robertson CE. Paramedics and technicians are equally successful at managing cardiac arrest outside hospital. BMJ 1995; 310:1091-1094.
doi: 10.1136/bmj.310.6987.1091 pmid: 7742673 |
| 30 |
Malzer R, Zeiner A, Binder M, Domanovits H, Knappitsch G, Sterz F, et al. Hemodynamic effects of active compression-decompression after prolonged CPR. Resuscitation 1996; 31:243-253.
pmid: 8783410 |
| 31 | Lafuente-Lafuente C, Melero-Bascones M. Active chest compression-decompression for cardiopulmonary resuscitation. Cochrane Database Syst Rev 2004; 2: CD002751. |
| 32 |
Plaisance P, Lurie KG, Vicaut E, Adnet F, Petit JL, Epain D, et al. A comparison of standard cardiopulmonary resuscitation and active compression-decompression resuscitation for out-of-hospital cardiac arrest. French Active Compression-Decompression Cardiopulmonary Resuscitation Study Group. N Engl J Med 1999; 341:569-575.
doi: 10.1056/NEJM199908193410804 pmid: 10451462 |
| [1] | Yu-qing Cui, Xian-fei Ding, Huo-yan Liang, Dong Wang, Xiao-juan Zhang, Li-feng Li, Quan-cheng Kan, Le-xin Wang, Tong-wen Sun. Efficacy and safety of low-dose corticosteroids for acute respiratory distress syndrome: A systematic review and meta-analysis [J]. World Journal of Emergency Medicine, 2021, 12(3): 207-213. |
| [2] | Xin Lu, Wei Han, Yan-xia Gao, Shi-gong Guo, Shi-yuan Yu, Xue-zhong Yu, Hua-dong Zhu, Yi Li. Efficacy and safety of corticosteroids in immunocompetent patients with septic shock [J]. World Journal of Emergency Medicine, 2021, 12(2): 124-130. |
| [3] | Xue-jie Dong, Lin Zhang, Yue-lin Yu, Shu-xiao Shi, Xiao-chen Yang, Xiao-qian Zhang, Shuang Tian, Helge Myklebust, Guo-hong Li, Zhi-jie Zheng. The general public’s ability to operate automated external defibrillator: A controlled simulation study [J]. World Journal of Emergency Medicine, 2020, 11(4): 238-245. |
| [4] | Alexei Birkun, Fatima Trunkwala, Adhish Gautam, Miriam Okoroanyanwu, Adesokan Oyewumi. Availability of basic life support courses for the general populations in India, Nigeria and the United Kingdom: An internet-based analysis [J]. World Journal of Emergency Medicine, 2020, 11(3): 133-139. |
| [5] | Shao-hua Liu, Huo-yan Liang, Hong-yi Li, Xian-fei Ding, Tong-wen Sun, Jing Wang. Effect of low high-density lipoprotein levels on mortality of septic patients: A systematic review and meta-analysis of cohort studies [J]. World Journal of Emergency Medicine, 2020, 11(2): 109-116. |
| [6] | Jung Wan Kim, Jin Woong Lee, Seung Ryu, Jung Soo Park, InSool Yoo, Yong Chul Cho, Hong Joon Ahn. Changes in peak inspiratory flow rate and peak airway pressure with endotracheal tube size during chest compression [J]. World Journal of Emergency Medicine, 2020, 11(2): 97-101. |
| [7] | Shi-yuan Yu, Yan-xia Gao, Joseph Walline, Xin Lu, Li-na Zhao, Yuan-xu Huang, Jiang Tao, An-yong Yu, Na Ta, Ren-ju Xiao, Yi Li. Role of penehyclidine in acute organophosphorus pesticide poisoning [J]. World Journal of Emergency Medicine, 2020, 11(1): 37-47. |
| [8] | Ye-cheng Liu, Yan-meng Qi, Hui Zhang, Joseph Walline, Hua-dong Zhu. A survey of ventilation strategies during cardiopulmonary resuscitation [J]. World Journal of Emergency Medicine, 2019, 10(4): 222-227. |
| [9] | Israel Olatunji Gabriel, Joel O. Aluko. Theoretical knowledge and psychomotor skill acquisition of basic life support training programme among secondary school students [J]. World Journal of Emergency Medicine, 2019, 10(2): 81-87. |
| [10] | Alexei Birkun, Yekaterina Kosova. Social attitude and willingness to attend cardiopulmonary resuscitation training and perform resuscitation in the Crimea [J]. World Journal of Emergency Medicine, 2018, 9(4): 237-248. |
| [11] | Alexei Birkun, Maksim Glotov, Herman Franklin Ndjamen, Esther Alaiye, Temidara Adeleke, Sergey Samarin. Pre-recorded instructional audio vs. dispatchers’ conversational assistance in telephone cardiopulmonary resuscitation: A randomized controlled simulation study [J]. World Journal of Emergency Medicine, 2018, 9(3): 165-171. |
| [12] | Alexei Birkun, Maksim Glotov. Education in cardiopulmonary resuscitation in Russia: A systematic review of the available evidence [J]. World Journal of Emergency Medicine, 2017, 8(4): 245-252. |
| [13] | Ling Zhou, Hui Li, Hong-yan Wei, Chun-lin Hu, Xiao-li Jing, Hong Zhan, Xiao-xing Liao, Xin Li. Study on the development and usage of a cardiopulmonary resuscitation time point recorder [J]. World Journal of Emergency Medicine, 2017, 8(3): 195-199. |
| [14] | Chennappa Kalvatala Krishna, Hakim Irfan Showkat, Meenakshi Taktani, Vikram Khatri. Out of hospital cardiac arrest resuscitation outcome in North India — CARO study [J]. World Journal of Emergency Medicine, 2017, 8(3): 200-205. |
| [15] | Vinej Somaraj, Rekha P Shenoy, Ganesh Shenoy Panchmal, Praveen S Jodalli, Laxminarayan Sonde, Ravichandra Karkal. Knowledge, attitude and anxiety pertaining to basic life support and medical emergencies among dental interns in Mangalore City, India [J]. World Journal of Emergency Medicine, 2017, 8(2): 131-135. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
