
Reduced Awareness for Osteoporosis in Distal Radius Fracture Patients Compared to Patients with Proximal Femur Fractures

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire
2.2. Self-Assessment of Health Status by Rating Scale
2.3. Osteoporosis Screening
3. Results
3.1. Questionnaire and Self-Assessment of Health Status by Rating Scale
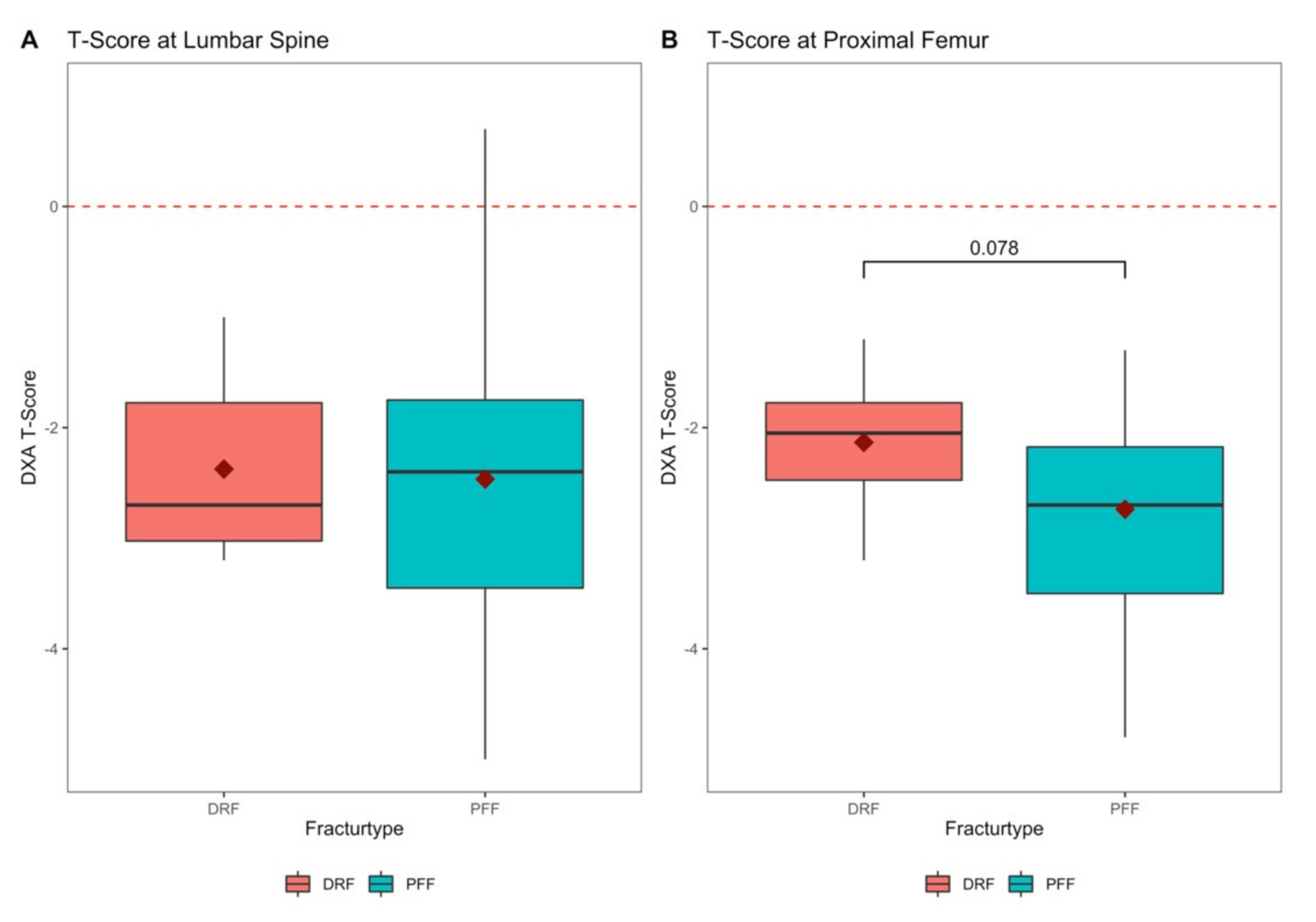
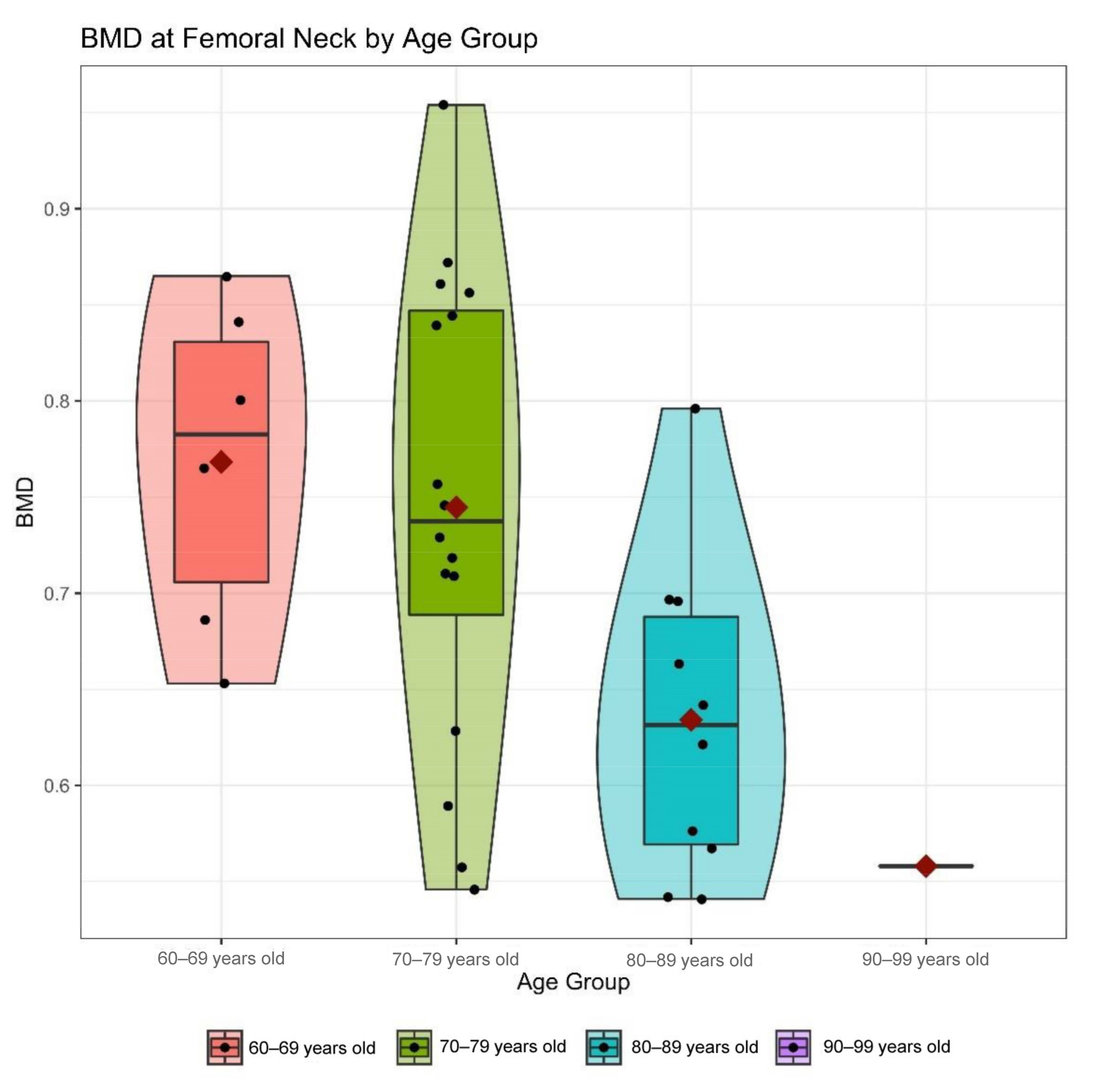
3.2. Testing for Osteoporosis and Bone Mineral Density
3.3. Patient’s Awareness for Osteoporosis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gibson-Smith, D.; Klop, C.; Elders, P.J.M.; Welsing, P.M.J.; van Schoor, N.; Leufkens, H.G.M.; Harvey, N.C.; van Staa, T.P.; de Vries, F. The risk of major and any (non-hip) fragility fracture after hip fracture in the United Kingdom: 2000–2010. Osteoporos. Int. 2014, 25, 2555–2563. [Google Scholar] [CrossRef]
- Sakuma, M.; Endo, N.; Oinuma, T.; Endo, E.; Yazawa, T.; Watanabe, K.; Watanabe, S. Incidence and outcome of osteoporotic fractures in 2004 in Sado City, Niigata Prefecture, Japan. J. Bone Miner. Metab. 2008, 26, 373–378. [Google Scholar] [CrossRef]
- Jupiter, J.B. Current concepts review. Fractures of the distal end of the radius. J. Bone Jt. Surg. Ser. A 1991, 73, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Jerrhag, D.; Englund, M.; Karlsson, M.K.; Rosengren, B.E. Epidemiology and time trends of distal forearm fractures in adults—a study of 11.2 million person-years in Sweden. BMC Musculoskelet. Disord. 2017, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuddihy, M.T.; Gabriel, S.E.; Crowson, C.S.; O’Fallon, W.M.; Melton, L.J. Forearm fractures as predictors of subsequent osteoporotic fractures. Osteoporos. Int. 1999, 9, 469–475. [Google Scholar] [CrossRef]
- Kanis, J.A.; Odén, A.; McCloskey, E.V.; Johansson, H.; Wahl, D.A.; Cooper, C. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos. Int. 2012, 23, 2239–2256. [Google Scholar] [CrossRef] [Green Version]
- Downey, C.; Kelly, M.; Quinlan, J.F. Changing trends in the mortality rate at 1-year post hip fracture—a systematic review. World J. Orthop. 2019, 10, 166–175. [Google Scholar] [CrossRef]
- Dyer, S.M.; Crotty, M.; Fairhall, N.; Magaziner, J.; Beaupre, L.A.; Cameron, I.D.; Sherrington, C. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, R.J.; Mahesri, M.; Abdia, Y.; Barberio, J.; Tong, A.; Zhang, D.; Mavros, P.; Kim, S.C.; Franklin, J.M. Association of Osteoporosis Medication Use After Hip Fracture With Prevention of Subsequent Nonvertebral Fractures: An Instrumental Variable Analysis. JAMA Netw. Open 2018, 1, e180826. [Google Scholar] [CrossRef]
- Saklad, M. Grading of Patients for Surgical Procedures. J. Am. Soc. Anesthesiol. 1941, 2, 281–284. [Google Scholar] [CrossRef]
- Doyle, D.J.; Goyal, A.; Bansal, P.; Garmon, E.H. American Society of Anesthesiologists Classification; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441940/ (accessed on 12 February 2021).
- Pfeilschifter, J. Osteoporose-Diagnostik: Was ist neu in der DVO-Leitlinie 2014? Dtsch. Med. Wochenschr. 2015, 140, 1667–1671. [Google Scholar] [CrossRef] [PubMed]
- Neuerburg, C.; Mittlmeier, L.; Schmidmaier, R.; Kammerlander, C.; Böcker, W.; Mutschler, W.; Stumpf, U. Investigation and management of osteoporosis in aged trauma patients: A treatment algorithm adapted to the German guidelines for osteoporosis. J. Orthop. Surg. Res. 2017, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boudreau, D.M.; Yu, O.; Balasubramanian, A.; Wirtz, H.; Grauer, A.; Crittenden, D.B.; Scholes, D. A Survey of Women’s Awareness of and Reasons for Lack of Postfracture Osteoporotic Care. J. Am. Geriatr. Soc. 2017, 65, 1829–1835. [Google Scholar] [CrossRef]
- Ziller, V.; Kostev, K.; Kyvernitakis, I.; Boeckhoff, J.; Hadji, P. Persistence and compliance of medications used in the treatment of osteoporosis—Analysis using a large scale, representative, longitudinal German database. Int. J. Clin. Pharmacol. Ther. 2012, 50, 315–322. [Google Scholar] [CrossRef]
- Murad, M.H.; Drake, M.T.; Mullan, R.J.; Mauck, K.F.; Stuart, L.M.; Lane, M.A.; Abu Elnour, N.O.; Erwin, P.J.; Hazem, A.; Puhan, M.A.; et al. Comparative effectiveness of drug treatments to prevent fragility fractures: A systematic review and network meta-analysis. J. Clin. Endocrinol. Metab. 2012, 97, 1871–1880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyun, S.G.; Won, S.O.; Moon, S.C.; Joo, H.O.; Young, H.L.; Goo, H.B. Patients with wrist fractures are less likely to be evaluated and managed for osteoporosis. J. Bone Jt. Surg. Ser. A 2009, 91, 2376–2380. [Google Scholar] [CrossRef]
- Kim, T.I.; Choi, J.H.; Kim, S.H.; Oh, J.H. The adequacy of diagnosis and treatment for osteoporosis in patients with proximal humeral fractures. CiOS Clin. Orthop. Surg. 2016, 8, 274–279. [Google Scholar] [CrossRef] [Green Version]
- Dimai, H.P.; Svedbom, A.; Fahrleitner-Pammer, A.; Resch, H.; Muschitz, C.; Thaler, H.; Szivak, M.; Amrein, K.; Borgström, F. Epidemiology of distal forearm fractures in Austria between 1989 and 2010. Osteoporos. Int. 2014, 25, 2297–2306. [Google Scholar] [CrossRef]
- Lippuner, K.; Von Overbeck, J.; Perrelet, R.; Bosshard, H.; Jaeger, P. Incidence and direct medical costs of hospitalizations due to osteoporotic fractures in Switzerland. Osteoporos. Int. 1997, 7, 414–425. [Google Scholar] [CrossRef]
- Ashe, M.; Khan, K.; Guy, P.; Kruse, K.; Hughes, K.; O’Brien, P.; Janssen, P.; McKay, H. Wristwatch—Distal radial fracture as a marker for osteoporosis investigation: A controlled trial of patient education and a physician alerting system. J. Hand Ther. 2004, 17, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Åkesson, K.E.; McGuigan, F.E.A. Closing the Osteoporosis Care Gap. Curr. Osteoporos. Rep. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gosch, M.; Kammerlander, C.; Neuerburg, C. Osteoporosis—Epidemiology and quality of care. Z. Gerontol. Geriatr. 2019, 52, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Geiger, I.; Kammerlander, C.; Höfer, C.; Volland, R.; Trinemeier, J.; Henschelchen, M.; Friess, T.; FLS-CARE study group; Böcker, W.; Sundmacher, L. Implementation of an integrated care programme to avoid fragility fractures of the hip in older adults in 18 Bavarian hospitals—study protocol for the cluster-randomised controlled fracture liaison service FLS-CARE. BMC Geriatr. 2021, 21, 43. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Results | |
|---|---|
| Age (in years; (%)) | 79.9 (8.6) |
| G1 (60–70 years) | 20 (13%) |
| G2 (71–79 years) | 54 (36%) |
| G3 (80–90 years) | 62 (41%) |
| G4 (91–100 years) | 14 (9%) |
| BMI (kg/m2) | 24.2 (±4.3) |
| <20 kg/m2 | 12 (8%) |
| 20–24.9 kg/m2 | 80 (53%) |
| 30–34.9 kg/m2 | 41 (27%) |
| 35–39.9 kg/m2 | 14 (9%) |
| ≥40 kg/m2 | 3 (2%) |
| ASA score | 3 (±0.6) |
| 1 | 7 (5%) |
| 2 | 59 (36%) |
| 3 | 80 (53%) |
| 4 | 4 (3%) |
| Risk Factors (DVO) | |
| Parental hip fracture | 48 (32%) |
| Current smoker | 13 (9%) |
| Glucocorticoid use | 18 12%) |
| Rheumatoid arthritis | 8 (5%) |
| Menopause <45 years | 46 (38%) |
| Aromatase inhibitor use | 10 (8%) |
| Alcohol (>1 bottle of beer a day) | 19 (13%) |
| Regular milk product consumption | 107 (71%) |
| Regular vitamin D intake | 34 (23%) |
| Known osteoporosis diagnosis | 36 (24%) |
| Osteoporosis medication intake | 23 (68%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keppler, A.M.; Kraus, M.; Blaschke, M.; Thomasser, N.; Kammerlander, C.; Böcker, W.; Neuerburg, C.; Stumpf, U.C. Reduced Awareness for Osteoporosis in Distal Radius Fracture Patients Compared to Patients with Proximal Femur Fractures. J. Clin. Med. 2021, 10, 848. https://doi.org/10.3390/jcm10040848
Keppler AM, Kraus M, Blaschke M, Thomasser N, Kammerlander C, Böcker W, Neuerburg C, Stumpf UC. Reduced Awareness for Osteoporosis in Distal Radius Fracture Patients Compared to Patients with Proximal Femur Fractures. Journal of Clinical Medicine. 2021; 10(4):848. https://doi.org/10.3390/jcm10040848
Chicago/Turabian StyleKeppler, Alexander Martin, Moritz Kraus, Matthias Blaschke, Nicole Thomasser, Christian Kammerlander, Wolfgang Böcker, Carl Neuerburg, and Ulla Cordula Stumpf. 2021. "Reduced Awareness for Osteoporosis in Distal Radius Fracture Patients Compared to Patients with Proximal Femur Fractures" Journal of Clinical Medicine 10, no. 4: 848. https://doi.org/10.3390/jcm10040848