
Health-Related Social and Ethical Considerations towards the Utilization of Dental Medical Services by Seniors: Influencing and Protective Factors, Vulnerability, Resilience and Sense of Coherence


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Results of the Selective Literature Search and Expert Panel
3.1.1. Influencing Factors for Non-Utilization of Dental Services by Older People
3.1.2. Vulnerability and Resilience in Older People
3.1.3. Salutogenesis and the Sense of Coherence—A Different Approach
3.1.4. Life Events in Old Age as a Risk Factor
3.2. Analysis of the Literature Search Conducted by the Expert Panel
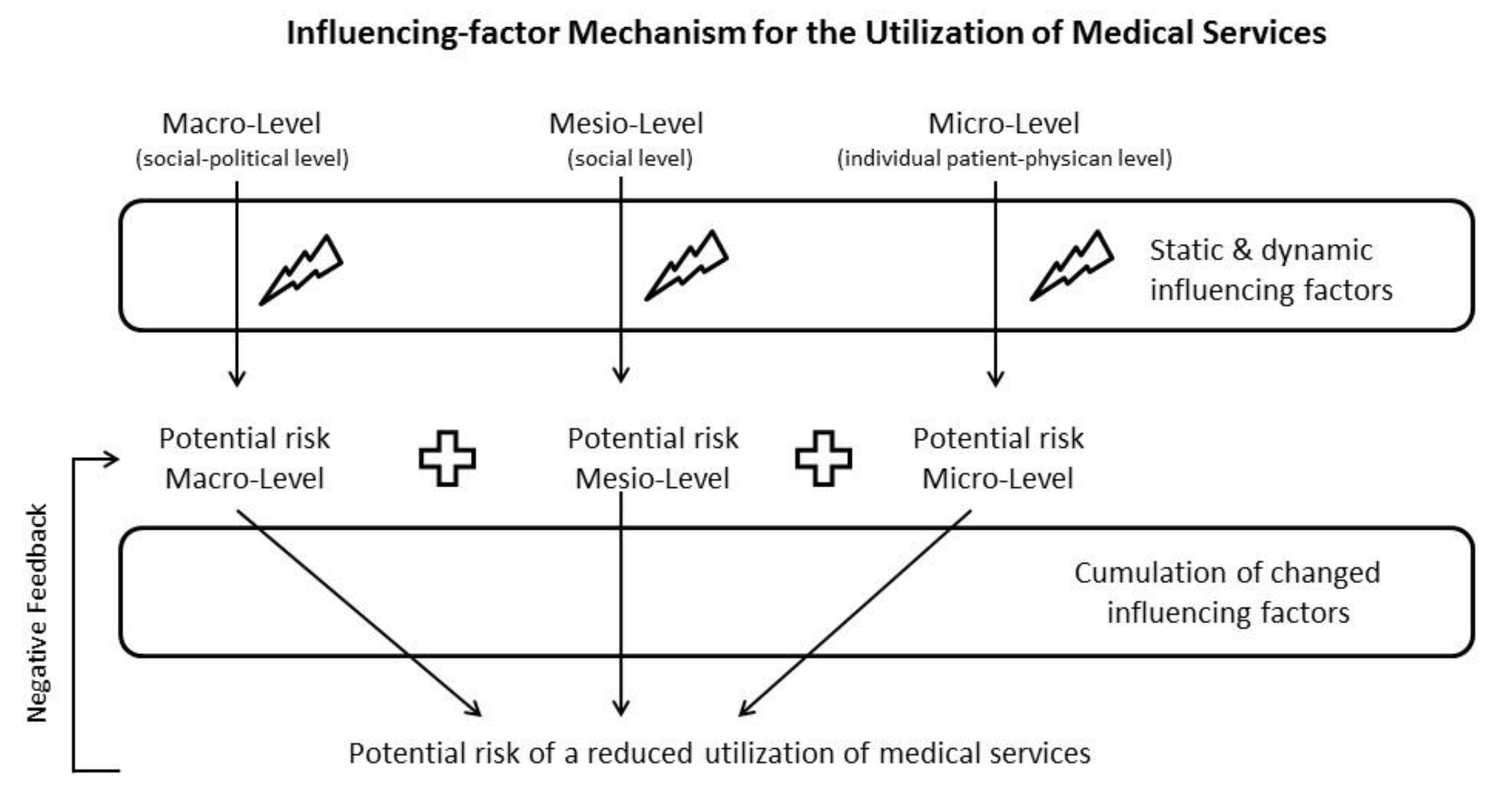
3.2.1. Factors Influencing the Use of Dental Services by Older People at the Various Levels of the Healthcare System and Their Influence Factor Mechanism
3.2.2. Protective Factors of the Utilization of Dental Healthcare Services
- Individual level;
- Social level;
- Social-political level.
3.3. Development of a New Terminology with Regard to Gerodontology
4. Discussion
4.1. Discussion of Findings
Influencing and Protective Factors
4.2. Health as Part of the Ageing Policy
4.3. Proposals for a Strategy for the Implementation of a Supportive Resilience Structure
4.4. Need for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andersen, R.M. A behavioral model of families’ use of health services. In Research Series; Center for Health Administration Studies, The University of Chicago: Chicago, IL, USA, 1968. [Google Scholar]
- Andersen, R.M.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. Milbank Q. 1973, 51, 95–124. [Google Scholar] [CrossRef] [Green Version]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- BFS—Swiss Federal Statistical Office. Statistics for Switzerland. Health and Health Behavior in Switzerland 2007. Swiss Health Survey; Federal Statistical Office: Neuchâtel, Switzerland, 2010. (In German)
- Nitschke, I.; Müller, F.; Hopfenmüller, W. The uptake of dental services by elderly Germans. Gerodontology 2001, 18, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Slack-Smith, L.; Hyndman, J. The relationship between demographic and health-related factors on dental service attendance by older Australians. Br. Dent. J. 2004, 197, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manski, R.J.; Moeller, J.; Chen, H.; St Clair, P.A.; Schimmel, J.; Magder, L.; Pepper, J.V. Dental care utilization and retirement. J. Public Health Dent. 2010, 70, 67–75. [Google Scholar] [CrossRef]
- Nitschke, I.; Stillhart, A.; Kunze, J. Utilization of dental services in old age. Swiss Dent. J. 2015, 125, 433–447. (In German) [Google Scholar] [PubMed]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 7th ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Nitschke, I.; Groß, D.; Kunze, J. Spezifische Bedarfe bei zahnärztlichen Patienten mit Demenz und ihre ethischen Implikationen. Ethik in der Medizin 2017, 29, 71–86. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar]
- Nitschke, I.; Hopfenmüller, W. Die Zahnmedizinische Versorgung älterer Menschen. [Dental care for older people.]. In The Berlin Aging Study; Mayer, K.U., Baltes, P.B., Eds.; Akademie Verlag: Berlin, Germany, 1996; pp. 429–448. (In German) [Google Scholar]
- Imfeld, T.; Lutz, F. The subjective evaluation of oral health in 40- to 69-year-old subjects. A representative survey of 600 persons in German and French-speaking Switzerland. Schweiz. Monatsschr. Zahnmed. 1995, 105, 1272–1283. [Google Scholar]
- Schimmel, M.; Schoeni, P.; Zulian, G.B.; Müller, F. Utilisation of dental services in a university hospital palliative and long-term care unit in Geneva. Gerodontology 2008, 25, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Plassman, B.L.; Liang, J.; Wei, L. Cognitive function and dental care utilization among community-dwelling older adults. Am. J. Public Health 2007, 97, 2216–2221. [Google Scholar] [CrossRef] [PubMed]
- AWMF. S3-Leitlinie Zahnbehandlungsangst, Langversion. Available online: https://www.awmf.org/uploads/tx_szleitlinien/083-020l_S3_Zahnbehandlungsangst-beim-Erwachsenen_2019-11.pdf (accessed on 16 January 2021).
- Freeman, R. Barriers to accessing dental care: Patient factor. Br. Dent. J. 1999, 187, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Borchelt, M. Prävention körperlicher Erkrankungen. In Angewandte Gerontologie in Schlüsselbegriffen; Wahl, H.-W., Tesch-Römer, C., Eds.; Kohlhammer Verlag: Stuttgart, Germany, 2000. [Google Scholar]
- Nitschke, I.; Kunze, J.; Hopfenmüller, W.; Reiber, T. Die zahnmedizinische funktionelle Kapazität—Ein Instrument in der Gerostomatologie. Quintessenz 2012, 63, 207–210. [Google Scholar]
- Bahadori, M.; Ravangard, R.; Asghari, B. Perceived Barriers Affecting Access to Preventive Dental Services: Application of DEMATEL Method. Iran. Red Crescent Med. J. 2013, 15, 655–662. [Google Scholar] [CrossRef] [Green Version]
- Bundesverfassungsgericht (BVerfG). Beschluss der 3. Kammer des Zweiten Senats vom 23. März 1998—2 BvR 2270/96-, Rn. 1-25. Available online: http://www.bverfg.de/e/rk19980323_2bvr227096.html (accessed on 16 January 2021).
- Stada Gesundheitsreport. Deutsche Patienten mit Wenig Vertrauen in Schulmedizin, Sprechende Medizin Steht Ganz Oben auf der Wunschliste der Patienten in Deutschland. Deutsche Ärztezeitschrift. Available online: https://www.aerztezeitung.de/Wirtschaft/Deutsche-Patienten-mit-wenig-Vertrauen-in-Schulmedizin-254820.html (accessed on 16 January 2021).
- Kiyak, H.A.; Reichmuth, M. Barriers to and enablers of older adults’ use of dental services. J. Dent. Educ. 2005, 69, 975–986. [Google Scholar] [CrossRef]
- Bundeszentrale für Politische Bildung. Regulierung des Gesundheitswesens in den Niederlanden. 2012. Available online: https://www.bpb.de/politik/innenpolitik/gesundheitspolitik/72976/regulierung#:~:text=Regulierung%20des%20Gesundheitswesens%20in%20den%20Niederlanden%201%20Ver%C3%A4nderte,Bedeutung%20der%20Verb%C3%A4nde.%20...%203%20Zunehmende%20Wettbewerbsorientierung (accessed on 12 February 2021).
- Wikipedia. Spanish National Health System. Available online: https://en.wikipedia.org/wiki/Spanish_National_Health_System#:~:text=Laws%20regulating%20the%20Spanish%20National%20Health%20System.%20The,of%20all%20citizens%20to%20protection%20of%20their%20health (accessed on 12 February 2021).
- Das österreichische Gesundheitssystem: Zahlen-Daten-Fakten (sozialministerium.at). Available online: https://broschuerenservice.sozialministerium.at/Home/Download?publicationId=636 (accessed on 12 February 2021).
- Gesundheitsgesetz (GesG). 2007. Available online: https://sgsm.ch/fileadmin/user_upload/Verbandsaerzte/Gesetzliche_Grundlagen/3.1.6_GesundheitsgesetzZH.pdf (accessed on 12 February 2021).
- European Commission. Cross-Border Healthcare. Directive 2011/24/EU. Available online: https://ec.europa.eu/health/cross_border_care/overview (accessed on 12 February 2021).
- Slack-Smith, L.; Lange, A.; Paley, G.; O’grady, M.; French, D.; Short, L. Oral health and access to dental care: A qualitative investigation among older people in the community. Gerodontology 2010, 27, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Nitschke, I.; Bär, C.; Hopfenmüller, W.; Roggendorf, H.; Stark, H.; Sobotta, B.; Reiber, T. Do long-term care residents benefit from the dental bonus system? Z. Gerontol. Geriatr. 2011, 44, 181–186. (In German) [Google Scholar] [CrossRef]
- National Health Service (NHS) UK. The NHS Longterm Plan. Available online: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf (accessed on 12 February 2021).
- Bachner, F.; Bobek, J.; Habimana, K.; Ladurner, J.; Lepuschutz, L.; Ostermann, H.; Rainer, L.; Schmidt, A.E.; Zuba, M.; Quentin, W.; et al. Austria: Health System Review. Health Syst. Transit. 2018, 20, 1–254. [Google Scholar]
- Bundesgesetzblatt. Gesetz zur Bekämpfung von Korruption im Gesundheitswesen. Available online: https://www.bgbl.de/xaver/bgbl/start.xav?startbk=Bundesanzeiger_BGBl&start=//*[@attr_id=%27bgbl116s1254.pdf%27]#__bgbl__%2F%2F*%5B%40attr_id%3D%27bgbl116s1254.pdf%27%5D__1613621145040 (accessed on 12 February 2021).
- Rock, K.S. Assessing the health-related dimensions of older adults’ social relationships. In Annual Review of Gerontology and Geriatrics; Lawton, M.P., Teresi, J.A., Eds.; Springer: New York, NY, USA, 1994; Volume 14, pp. 142–181. [Google Scholar]
- Baltes, M.M.; Silverberg, S.B. The dynamics between dependency and autonomy: Illustrations across the life span. Life-Span Dev. Behav. 1994, 12, 41–90. [Google Scholar]
- Schröder-Butterfill, E.; Marianti, R. A framework for understanding old-age vulnerabilities. Ageing Soc. 2006, 26, 9–35. [Google Scholar] [CrossRef] [Green Version]
- Sieber, C. Frailty (Gebrechlichkeit). In Praxishandbuch Altersmedizin: Geriatrie–Gerontopsychiatrie–Gerontologie; Pantel, J., Schröder, J., Bollheimer, C., Kruse, A., Eds.; Kohlhammer: Stuttgart, Germany, 2007; pp. 84–93. [Google Scholar]
- Bürkner, H.J. Vulnerabilität und Resilienz—Forschungsstand und Sozialwissenschaftliche Untersuchungsperspektiven (Working Paper); Leibniz-Institut für Regionalentwicklung und Strukturplanung IRS: Erkner, Germany; Available online: https://d-nb.info/1028582749/34 (accessed on 16 January 2021).
- Staudinger, U.; Marsiske, M.; Baltes, P.B. Resilience and reserve capacity in later adulthood: Potentials and limits of development across lif span. In Developmental Psychopathology; Cicchetti, D., Cohen, D.J., Eds.; Wiley: Hoboken, NJ, USA, 2006; Volume 2, pp. 801–847. [Google Scholar]
- Jordan, R.A.; Bodechtel, C.; Hertrampf, K.; Hoffmann, T.; Kocher, T.; Nitschke, I.; Schiffner, U.; Stark, H.; Zimmer, S.; Micheelis, W. The Fifth German Oral Health Study (Fünfte Deutsche Mundgesundheitsstudie, DMS V)-rationale, design, and methods. BMC Oral Health 2014, 14, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well; Jossey-Bass Publishers: San Francisco, CA, USA, 1987. [Google Scholar]
- Singer, S. Salutogenese in der Zahnmedizin. IDZ-Information 2010, 4, 1–26. [Google Scholar]
- Micheelis, W.; Nitschke, I. Profile des Sense of Coherence (SOC) bei Jüngeren Erwachsenen und Jüngeren Senioren. In Institut der Deutschen Zahnärzte (IDZ) (Hrsg.) Fünfte Deutsche Mundgesundheitsstudie (DMS V); Jordan, R., Micheelis, W., Eds.; Deutscher Zahnärzte Verlag DÄV: Köln, Germany, 2016; pp. 579–589. ISBN 978-3-7691-0020-4. [Google Scholar]
- Singer, S.; Brähler, E. Die “Sense of Coherence Scale”. Testhandbuch zur Deutschen Version; Vandenhoeck & Ruprecht: Göttingen, Germany, 2014; pp. 9–10. ISBN 9783647491264. [Google Scholar]
- Eriksson, M.; Mittelmark, M.B. The Sense of Coherence and its Measurement 12. In the Handbook of Salutogenesis; Springer: Berlin/Heidelberg, Germany, 2017; Volume 97. [Google Scholar]
- Martin, M.; Kliegel, M. Grundriss Gerontologie Band 3. Psychologische Grundlagen der Gerontologie. Anwendungsfelder der Gerontopsychologie; Kohlhammer Urban: Stuttgart, Germany, 2010; p. 288. ISBN 978-3-17-021445-3. [Google Scholar]
- Schiffner, U. Krankheits- und Versorgungsprävalenzen bei jüngeren Senioren (65-bis 74-Jährige). Karies und Erosionen. In Fünfte Deutsche Mundgesundheitsstudie; Jordan, A.R., Micheelis, W., Eds.; Deutscher Ärzte-Verlag: Köln, Germany, 2016; pp. 363–395. ISBN 978-3-7691-0020-4. [Google Scholar]
- Schiffner, U. Krankheits- und Versorgungsprävalenzen bei älteren Senioren (75-bis 100-Jährige). Karies und Erosionen. In Fünfte Deutsche Mundgesundheitsstudie; Jordan, A.R., Micheelis, W., Eds.; Deutscher Ärzte-Verlag: Köln, Germany, 2016; pp. 475–502. ISBN 978-3-7691-0020-4. [Google Scholar]
- Schulz-Nieswandt, F. Grundriss Gerontologie Band 5. Sozialpolitik und Alter(n). Gegenwartsprobleme der Alterssozialpolitik; Kohlhammer Urban: Stuttgart, Germany, 2007; p. 173. ISBN 978-3-17-018142-7. (In German) [Google Scholar]
- Magnus, D. Fürsorge oder Selbstbestimmung? Dtsch. Ärzteblatt 2012, 109, 913–918. [Google Scholar]
- Nitschke, I. Zur Mundgesundheit von Senioren—Ein Epidemiologischer Überblick über Ausgewählte Oro-Faziale Erkrankungen und Ihre Longitudinale Betrachtung, Habilitationsschrift, University Leipzig. Habilitationsschriften der Zahn-, Mund- und Kieferheilkunde; Quintessenz-Verlag: Berlin, Germany, 2006; ISBN 3-87652-898-4. [Google Scholar]
- Kruse, A. Grundriss Gerontologie Band 21. Das Letzte Lebensjahr. Zur Körperlichen, Psychischen und Sozialen Situation des Alten Menschen am Ende Seines Lebens. Der Freitod—Eine Kritische Stellungnahme; Kohlhammer Urban: Stuttgart, Germany, 2007; p. 194. [Google Scholar]
- Beise, U. Prävention und Gesundheitsförderung. In Gesundheits- und Krankheitslehre; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]


{kind=link}
| Levels | Parties | Static Factors | Dynamic Factors |
|---|---|---|---|
| Macro Level (social-political level) | Population |
|
|
| Mesio Level (social level) | Population Non-healthy peopleHealth-insured people |
|
|
| Micro Level (individual patient–physican level) | Patients | Objective influencing factors
| |
| Dentist |
|
| |
| Patient–Dentist |
|
|
| Protective Factors of Utilization—Patient-Specific Factors | |
|---|---|
| Individual Level (Micro Level Patient) |
|
| Protective Factors of Utilization—Others Than Patient-Specific Factors | |
|---|---|
| Individual Level (Micro Level Dentist) Dentist/team dependent qualities | Gerostomatological “feel-good factor” of the dental office
|
| Social Level Internal support level Internal, social support by family/relatives and the population |
|
| Social Level External support level External, social support (caregivers/volunteers/physicians) |
|
| Social–Political Level |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nitschke, I.; Hahnel, S.; Jockusch, J. Health-Related Social and Ethical Considerations towards the Utilization of Dental Medical Services by Seniors: Influencing and Protective Factors, Vulnerability, Resilience and Sense of Coherence. Int. J. Environ. Res. Public Health 2021, 18, 2048. https://doi.org/10.3390/ijerph18042048
Nitschke I, Hahnel S, Jockusch J. Health-Related Social and Ethical Considerations towards the Utilization of Dental Medical Services by Seniors: Influencing and Protective Factors, Vulnerability, Resilience and Sense of Coherence. International Journal of Environmental Research and Public Health. 2021; 18(4):2048. https://doi.org/10.3390/ijerph18042048
Chicago/Turabian StyleNitschke, Ina, Sebastian Hahnel, and Julia Jockusch. 2021. "Health-Related Social and Ethical Considerations towards the Utilization of Dental Medical Services by Seniors: Influencing and Protective Factors, Vulnerability, Resilience and Sense of Coherence" International Journal of Environmental Research and Public Health 18, no. 4: 2048. https://doi.org/10.3390/ijerph18042048