
Lower Prevalence of Atopic Dermatitis and Allergic Sensitization among Children and Adolescents with a Two-Sided Migrant Background

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Data Collection and Analysis
3. Results
3.1. Basic Characteristics of the Study Population
3.2. Main Findings
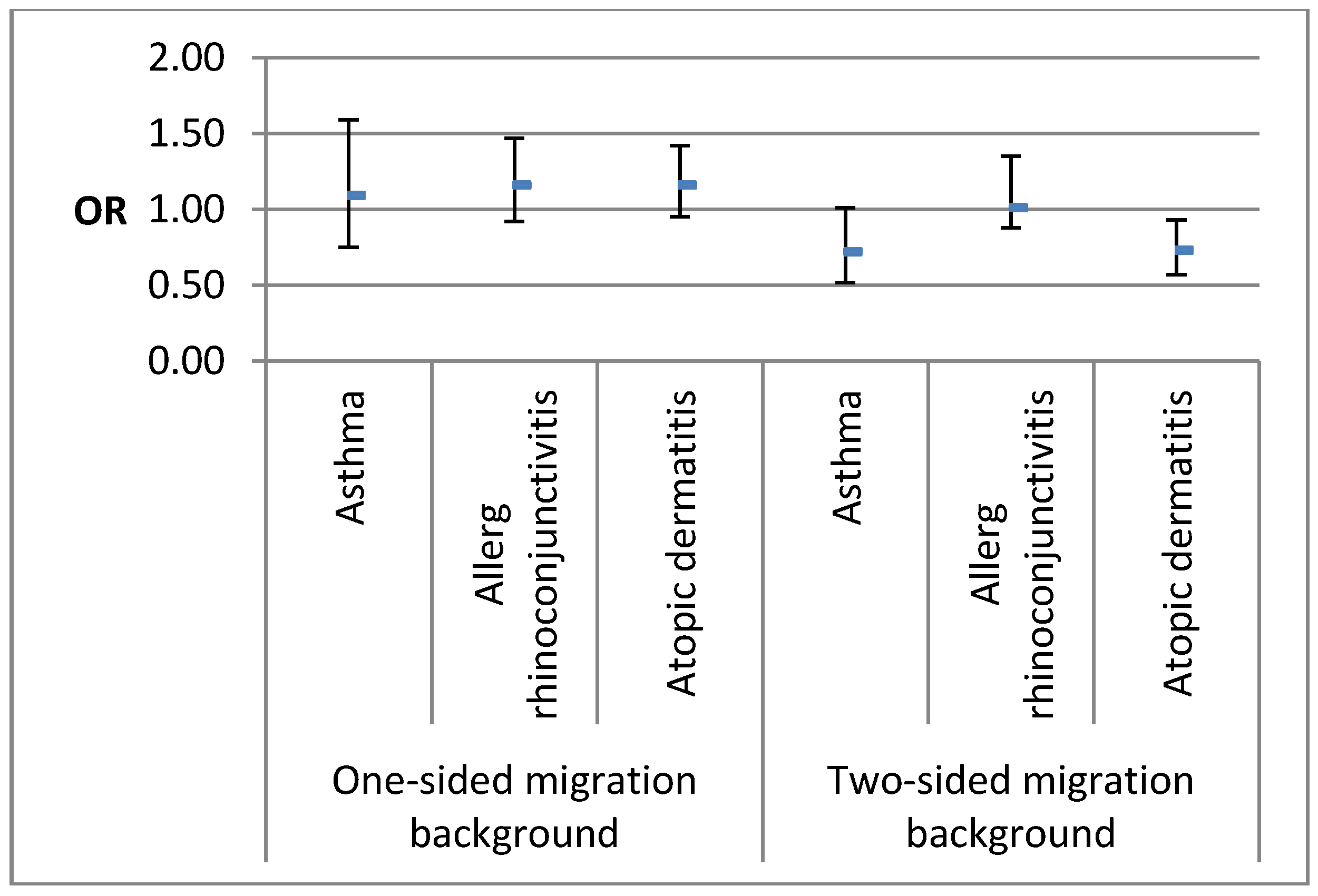
3.2.1. Atopic Diseases
3.2.2. Allergic Sensitization
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| CAPI | Computer Assisted Personal Interview |
| KiGGS | German Health Interview and Examination Survey for children and adolescents |
| NHANESIII | Third National Health and Nutrition Examination Survey |
| NHIS | National Health Interview Survey |
| OR | Odds Ratio |
| RKI | Robert Koch Institute |
| WHO | World Health Organization |
References
- Galassi, C.; De Sario, M.; Biggeri, A.; Bisanti, L.; Chellini, E.; Ciccone, G.; Petronio, M.G.; Piffer, S.; Sestini, P.; Rusconi, F.; et al. Changes in prevalence of asthma and allergies among children and adolescents in Italy: 1994–2002. Pediatrics 2006, 117, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Horii, K.A.; Simon, S.D.; Liu, D.Y.; Sharma, V. Atopic dermatitis in children in the United States, 1997–2004: Visit trends, patient and provider characteristics, and prescribing patterns. Pediatrics 2007, 120, e527–e534. [Google Scholar] [CrossRef] [PubMed]
- Grize, L.; Gassner, M.; Wüthrich, B.; Bringolf-Isler, B.; Takken-Sahli, K.; Sennhauser, F.; Stricker, T.; Eigenmann, P.; Braun-Fahrländer, C. Trends in prevalence of asthma, allergic rhinitis and atopic dermatitis in 5–7-year old Swiss children from 1992 to 2001. Allergy 2006, 61, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Mortz, C.; Lauritsen, J.; Bindslev-Jensen, C.; Andersen, K.E. Prevalence of atopic dermatitis, asthma, allergic rhinitis, and hand and contact dermatitis in adolescents. The Odense Adolescence Cohort Study on Atopic Diseases and Dermatitis. Br. J. Dermatol. 2001, 144, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Visness, C.M.; London, S.J.; Daniels, J.L.; Kaufman, J.S.; Yeatts, K.B.; Siega-Riz, A.M.; Calatroni, A.; Zeldin, D.C. Association of childhood obesity with atopic and nonatopic asthma: Results from the National Health and Nutrition Examination Survey 1999–2006. J. Asthma 2010, 47, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Wuthrich, B.; Schmid-Grendelmeier, P. The atopic eczema/dermatitis syndrome. Epidemiology, natural course, and immunology of the IgE-associated (“extrinsic”) and the nonallergic (“intrinsic”) AEDS. J. Investig. Allergol. Clin. Immunol. 2003, 13, 1–5. [Google Scholar] [PubMed]
- Schernhammer, E.S.; Vutuc, C.; Waldhor, T.; Haidinger, G. Time trends of the prevalence of asthma and allergic disease in Austrian children. Pediatr. Allergy Immunol. 2008, 19, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, H.F.; Eller, E.; Host, A.; Andersen, K.E.; Bindslev-Jensen, C. The prevalence of allergic diseases in an unselected group of 6-year-old children. The DARC birth cohort study. Pediatr. Allergy. Immunol. 2008, 19, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Hurrelmann, K. Jugendgesundheitssurvey: Internationale Vergleichsstudie im Auftrag der Weltgesundheitsorganisation WHO; Juventa-Verlag: Weinheim and Munich, Germany, 2003. [Google Scholar]
- Kamtsiuris, P.; Lange, M.; Schaffrath, R.A. The German Health Interview and Examination Survey for Children and Adolescents (KiGGS): Sample design, response and nonresponse analysis. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2006, 50, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Kurth, B.-M.; Kamtsiuris, P.; Hölling, H.; Schlaud, M.; Dölle, R.; Ellert, U.; Kahl, H.; Knopf, H.; Lange, M.; Mensink, G.B. The challenge of comprehensively mapping children’s health in a nation-wide health survey: Design of the German KiGGS-Study. BMC. Public Health 2008, 8, 196. [Google Scholar] [CrossRef] [PubMed]
- Holling, H.; Kamtsiuris, P.; Lange, M.; Thierfelder, W.; Thamm, M.; Schlack, R. The German Health Interview and Examination Survey for Children and Adolescents (KiGGS): Study management and conduct of fieldwork. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 557–566. [Google Scholar] [PubMed]
- Schenk, L.; Ellert, U.; Neuhauser, H. Children and adolescents in Germany with a migration background. Methodical aspects in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Kamtsiuris, P.; Lange, C.; Schaffrath Rosario, A.; Stolzenberg, H.; Lampert, T. Sociodemographic characteristics in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS)—Operationalisation and public health significance, taking as an example the assessment of general state of health. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Winkler, J.; Stolzenberg, H. Der Sozialschichtindex im Bundes-Gesundheitssurvey. Gesundheitswesen 1999, 61, 178–183. [Google Scholar]
- Kucukosmanoglu, E.; Yazi, D.; Yesil, O.; Akkoc, T.; Gezer, M.; Ozdemir, C.; Bakirci, N.; Bahceciler, N.N.; Barlan, I.B. Prevalence of immediate hypersensitivity reactions to cow’s milk in infants based on skin prick test and questionnaire. Allergol. Immunopathol. 2008, 36, 254–258. [Google Scholar] [CrossRef]
- Jarvinen, K.M.; Suomalainen, H. Development of cow’s milk allergy in breast-fed infants. Clin. Exp. Allergy 2001, 31, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Eggesbo, M.; Botten, G.; Halvorsen, R.; Magnus, P. The prevalence of CMA/CMPI in young children: The validity of parentally perceived reactions in a population-based study. Allergy 2001, 56, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Grüber, C.; Meinlschmidt, G.; Bergmann, R.; Wahn, U.; Stark, K. Is early BCG vaccination associated with less atopic disease? An epidemiological study in German preschool children with different ethnic backgrounds. Pediatr. Allergy Immunol. 2002, 13, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Grüber, C.; Illi, S.; Plieth, A.; Sommerfeld, C.; Wahn, U. Cultural adaptation is associated with atopy and wheezing among children of Turkish origin living in Germany. Clin. Exp. Allergy 2002, 32, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Kabesch, M.; Schaal, W.; Nicolai, T.; Von Mutius, E. Lower prevalence of asthma and atopy in Turkish children living in Germany. Eur. Respir. J. 1999, 13, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Apfelbacher, C.J.; Diepgen, T.L.; Schmitt, J. Determinants of eczema: Population-based cross-sectional study in Germany. Allergy 2011, 66, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, A.; Barcella, M.; Bo, G.A.; Miadonna, A. Onset of allergy and asthma symptoms in extra-European immigrants to Milan, Italy: Possible role of environmental factors. Clin. Exp. Allergy 2003, 33, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Marcon, A.; Cazzoletti, L.; Rava, M.; Gisondi, P.; Pironi, V.; Ricci, P.; De Marco, R. Incidence of respiratory and allergic symptoms in Italian and immigrant children. Respir. Med. 2011, 105, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Farfel, A.; Green, M.S.; Shochat, T.; Noyman, I.; Levy, Y.; Afek, A. Trends in specific morbidity prevalence in male adolescents in Israel over a 50 year period and the impact of recent immigration. Isr. Med. Assoc. J. 2007, 9, 149–152. [Google Scholar] [PubMed]
- Leung, R.C.; Carlin, J.B.; Burdon, J.G.; Czarny, D. Asthma, allergy and atopy in Asian immigrants in Melbourne. Med. J. Aust. 1994, 161, 418–425. [Google Scholar]
- Silverberg, J.I.; Simpson, E.L.; Durkin, H.G.; Joks, R. Prevalence of allergic disease in foreign-born American children. JAMA Pediatr. 2013, 167, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Holguin, F.; Mannino, D.M.; Anto, J.; Mott, J.; Ford, E.S.; Teague, W.G.; Redd, S.C.; Romieu, I. Country of birth as a risk factor for asthma among Mexican Americans. Am. J. Respir. Crit. Care. Med. 2005, 171, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Eldeirawi, K.; McConnell, R.; Freels, S.; Persky, V.W. Associations of place of birth with asthma and wheezing in Mexican American children. J. Allergy. Clin. Immunol. 2005, 116, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Brugge, D.; Lee, A.C.; Woodin, M.; Rioux, C. Native and foreign born as predictors of pediatric asthma in an Asian immigrant population: A cross sectional survey. Environ. Health 2007, 6, 13. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.G.; Henry, R.L.; Shah, S.; Powell, H.; Wang, H. Migration to a western country increases asthma symptoms but not eosinophilic airway inflammation. Pediatr. Pulmonol. 2003, 36, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Rottem, M.; Szyper-Kravitz, M.; Shoenfeld, Y. Atopy and asthma in migrants. Int. Arch. Allergy. Immunol. 2005, 136, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Leung, R. Asthma and migration. Respirology 1996, 1, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Coultas, D.B.; Gong, H., Jr.; Grad, R.; Handler, A.; McCurdy, S.A.; Player, R.; Rhoades, E.R.; Samet, J.M.; Thomas, A.; Westley, M. Respiratory diseases in minorities of the United States. Am. J. Respir. Crit. Care. Med. 1994, 149, S93–S131. [Google Scholar] [CrossRef] [PubMed]
- Spallek, J.; Zeeb, H.; Razum, O. Prevention among immigrants: The example of Germany. BMC Public Health 2010, 10, 92. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.A.; Saboor, H.T.; Qayyum, Z.; Khan, I.; Habib, Z.; Waheed, H.T. Barriers to accessing the German health-care system for Pakistani immigrants in Berlin, Germany: A qualitative exploratory study. Lancet 2013, 382, 18. [Google Scholar] [CrossRef]
- Henderson, S.; Kendall, E. Culturally and linguistically diverse peoples’ knowledge of accessibility and utilisation of health services: Exploring the need for improvement in health service delivery. Aust. J. Prim. Health 2011, 17, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Povlsen, L.; Olsen, B.; Ladelund, S. Diabetes in children and adolescents from ethnic minorities: Barriers to education, treatment and good metabolic control. J. Adv. Nurs. 2005, 50, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.M.; Cullinan, P.; Williams, H.; Mills, P.; Moffat, S.; White, C.; Newman, T.A. Environmental associations with eczema in early life. Br. J. Dermatol. 2001, 144, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.M.; Gelfand, J.M.; Yan, A.C. The epidemiology of atopic dermatitis. Clin. Dermatol. 2003, 21, 109–115. [Google Scholar] [CrossRef]
- Schmitz, R.; Atzpodien, K.; Schlaud, M. Prevalence and risk factors of atopic diseases in German children and adolescents. Pediatr. Allergy. Immunol. 2012, 23, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Strachan, D.P. Hay fever, hygiene, and household size. BMJ 1989, 299, 1259–1260. [Google Scholar] [CrossRef] [PubMed]
- Karmaus, W.; Botezan, C. Does a higher number of siblings protect against the development of allergy and asthma? A review. J. Epidemiol. Community Health 2002, 56, 209–217. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Migrant Background | |||
|---|---|---|---|---|
| Basic Characteristics | n = 17,450 % (n) * | Two-Sided n = 2580 % (n) * | One-Sided n = 1283 % (n) * | None n = 13,507 % (n) * |
| Sex | ||||
| Male | 51.3 (8880) | 52.1 (1350) | 52.5 (656) | 51.0 (6842) |
| Female | 48.7 (8570) | 47.9 (1230) | 47.5 (627) | 49.0 (6665) |
| Age group (in years) | ||||
| 0–2 | 13.6 (2770) | 12.7 (360) | 19.9 (279) | 13.0 (2113) |
| 3–6 | 21.0 (3832) | 21.5 (565) | 24.2 (315) | 20.5 (2920) |
| 7–10 | 21.7 (4107) | 21.3 (606) | 21.8 (306) | 21.8 (3169) |
| 11–13 | 17.3 (3040) | 18.9 (486) | 14.8 (185) | 17.3 (2369) |
| 14–17 | 26.3 (3701) | 25.6 (563) | 19.4 (198) | 27.4 (2936) |
| Socio-economic status | ||||
| High | 27.1 (4366) | 10.0 (217) | 30.3 (376) | 30.2 (3143) |
| Middle | 45.4 (7901) | 36.3 (834) | 42.7 (538) | 47.6 (6507) |
| Low | 27.5 (4760) | 53.7 (1250) | 27.0 (356) | 22.1 (3764) |
| Living environment | ||||
| Rural | 45.3 (8463) | 24.2 (631) | 31.3 (429) | 51.7 (7365) |
| Urban | 54.7 (8987) | 75.8 (1949) | 68.7 (854) | 48.3 (6142) |
| Parental atopy | ||||
| Yes | 37.9 (7341) | 25.1 (579) | 39.5 (487) | 40.5 (5174) |
| No | 62.1 (9372) | 74.9 (1772) | 60.5 (792) | 59.5 (8212) |
| Mold-infested rooms | ||||
| Yes | 5.1 (893) | 9.9 (245) | 5.4 (72) | 4.1 (575) |
| No | 94.9 (16,199) | 90.1 (2100) | 94.6 (1204) | 95.9 (12,853) |
| Smoking mother and/or father | ||||
| Yes | 49.8 (8716) | 54.6 (1380) | 53.2 (692) | 48.3 (6617) |
| No | 50.2 (8479) | 45.4 (1121) | 46.8 (692) | 51.7 (6758) |
| Birth order | ||||
| Last or middle born | 49.8 (8156) | 54.2 (1159) | 44.2 (552) | 49.5 (6441) |
| First born, as part of multiples or w/o siblings | 50.2 (8291) | 45.8 (972) | 55.8 (687) | 50.5 (6629) |
| Atopic Disease | Migrant Background | |||||
|---|---|---|---|---|---|---|
| None | One-Sided | Two-Sided | ||||
| % (95%-CI) * | N ** | % (95%-CI) * | N ** | % (95%-CI) * | N ** | |
| Lifetime prevalence | ||||||
| Asthma | 4.7 (4.3–5.1) | 593 | 5.9 (4.6–7.4) | 70 | 4.4 (3.7–5.2) | 107 |
| Allergic rhinoconjunctivitis | 11.0 (10.3–11.7) | 1339 | 11.1 (9.3–13.2) | 129 | 9.6 (8.3–10.9) | 232 |
| Atopic dermatitis | 14.4 (13.6–15.3) | 1920 | 13.4 (11.6–15.3) | 174 | 8.0 (7.0–9.1) | 210 |
| p ≤ 0.0001 | ||||||
| 12-month prevalence | ||||||
| Asthma | 3.1 (2.7–3.4) | 381 | 3.5 (2.6–4.7) | 42 | 2.4 (1.9–3.1) | 61 |
| Allergic rhinoconjunctivitis | 9.0 (8.4–9.6) | 1101 | 9.2 (7.6–11.0) | 104 | 7.7 (6.8–8.8) | 189 |
| Atopic dermatitis | 7.7 (7.1–8.3) | 1069 | 8.6 (7.3–10.3) | 113 | 4.6 (3.8–5.6) | 121 |
| p ≤ 0.0001 | ||||||
| n = 13,100 | Migrant Background | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| None | One-Sided | Two-Sided | ||||||
| % (95%-CI) * | N ** | % (95%-CI) * | N ** | % (95%-CI) * | N ** | % (95%-CI) * | N ** | |
| Sensitized to at least one of the test allergens | 40.3 (38.9–41.7) | 4006 | 42.9 (38.9–47.0) | 369 | 39.1 (36.9–41.4) | 735 | 40.3 (38.9–41.5) | 5110 |
| Cladosporium herbarum (mold) | 1.8 (1.5–2.1) | 198 | 2.5 (1.7–3.9) | 22 | 1.2 (0.8–1.9) | 22 | 1.7 (1.5–2.0) | 245 |
| Aspergillus fumigatus (mold) | 2.3 (1.9–2.6) | 255 | 2.6 (1.8–3.8) | 24 | 2.4 (1.8–3.3) | 46 | 2.3 (2.0–2.7) | 327 |
| Egg white (food) | 4.7 (4.2–5.2) | 472 | 6.6 (5.0–8.8) | 56 | 5.5 (4.5–6.7) | 106 | 5.0 (4.5–5.5) | 637 |
| Cow’s milk protein(food) | 5.3 (4.8–5.9) | 523 | 6.8 (5.0–9.1) | 59 | 7.1 (6.0–8.4) | 138 | 5.8 (5.2–6.3) | 725 |
| Soybean (food) | 7.0 (6.2–7.9) | 684 | 5.0 (3.7–6.7) | 43 | 4.0 (3.1–5.2) | 77 | 6.3 (5.6–7.1) | 806 |
| Rice (food) | 8.0 (7.1–9.0) | 794 | 5.5 (4.1–7.4) | 47 | 4.2 (3.3–5.5) | 86 | 7.2 (6.4–8.0) | 930 |
| Potato (food) | 9.3 (8.3–10.4) | 900 | 7.3 (5.5–9.7) | 59 | 5.2 (4.1–6.5) | 98 | 8.4 (7.5–9.3) | 1059 |
| Apple (food) | 9.9 (9.0–10.9) | 964 | 9.5 (7.6–11.9) | 80 | 6.1 (4.9–7.5) | 119 | 9.2 (8.5–10.0) | 1167 |
| Carrot (food) | 10.4 (9.5–11.4) | 1014 | 9.6 (7.6–12.0) | 80 | 6.6 (5.4–8.0) | 129 | 9.7 (8.9–10.5) | 1228 |
| Wheat (food) | 10.6 (9.6–11.6) | 1050 | 8.6 (6.6–11.0) | 71 | 7.4 (6.1–8.9) | 141 | 9.9 (9.0–10.7) | 1266 |
| Peanut (food) | 11.6 (10.5–12.7) | 1150 | 9.7 (7.8–12.0) | 81 | 7.0 (5.8–8.5) | 134 | 10.6 (9.7–11.6) | 1369 |
| Mugwort (pollen) | 11.6 (10.7–12.6) | 1199 | 10 (8.0–12.4) | 85 | 8.0 (6.6–9.6) | 152 | 10.8 (10.0–11.7) | 1440 |
| Common silver birch (pollen) | 14.9 (13.9–16.0) | 1483 | 15.9 (13.5–18.6) | 131 | 9.7 (8.4–11.3) | 184 | 14.1 (13.2–15.0) | 1806 |
| Cultivated rye (pollen) | 22.0 (20.6–23.4) | 2175 | 21.7 (18.7–25.0) | 182 | 17.4 (15.6–19.5) | 334 | 21.1 (20.0–22.3) | 2701 |
| Timothy grass (pollen) | 23.4 (22.1–24.8) | 2322 | 23.3 (20.1–26.9) | 199 | 19.4 (17.5–21.5) | 365 | 22.7 (21.5–23.9) | 2899 |
| Horse dander (animal) | 4.8 (4.3–5.3) | 476 | 4.7 (3.4–6.6) | 40 | 2.5 (2.0–3.2) | 51 | 4.4 (4.0–4.8) | 569 |
| Cat dander (animal) | 8.5 (7.9–9.2) | 894 | 8.6 (6.7–11.1) | 71 | 6.1 (5.0–7.4) | 71 | 8.1 (7.6–8.7) | 1088 |
| Dog dander (animal) | 10.2 (9.5–11.0) | 1022 | 8.3 (6.5–10.5) | 72 | 7.7 (6.4–9.2) | 149 | 9.6 (9.1–10.3) | 1249 |
| Dermatophagoides farina (house dust mite) | 21.0 (20.1–22.0) | 2077 | 19.4 (16.5–22.7) | 165 | 20.0 (18.1–22.0) | 373 | 20.7 (19.9–21.6) | 2627 |
| Dermatophagoides pteronyssinus (house dust mite) | 21.0 (20.1–21.9) | 2085 | 19.7 (16.6–23.2) | 170 | 21.1 (19.3–23.0) | 395 | 20.9 (20.1–21.8) | 2661 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ernst, S.A.; Schmitz, R.; Thamm, M.; Ellert, U. Lower Prevalence of Atopic Dermatitis and Allergic Sensitization among Children and Adolescents with a Two-Sided Migrant Background. Int. J. Environ. Res. Public Health 2016, 13, 265. https://doi.org/10.3390/ijerph13030265
Ernst SA, Schmitz R, Thamm M, Ellert U. Lower Prevalence of Atopic Dermatitis and Allergic Sensitization among Children and Adolescents with a Two-Sided Migrant Background. International Journal of Environmental Research and Public Health. 2016; 13(3):265. https://doi.org/10.3390/ijerph13030265
Chicago/Turabian StyleErnst, Sinja Alexandra, Roma Schmitz, Michael Thamm, and Ute Ellert. 2016. "Lower Prevalence of Atopic Dermatitis and Allergic Sensitization among Children and Adolescents with a Two-Sided Migrant Background" International Journal of Environmental Research and Public Health 13, no. 3: 265. https://doi.org/10.3390/ijerph13030265