Development of Case Numbers during the COVID-19 Pandemic in a Center of Maximum-Care for Traumatology and Orthopedic Oncology


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Ethics
2.3. Examination Parameters
2.4. Statistical Analysis
3. Results
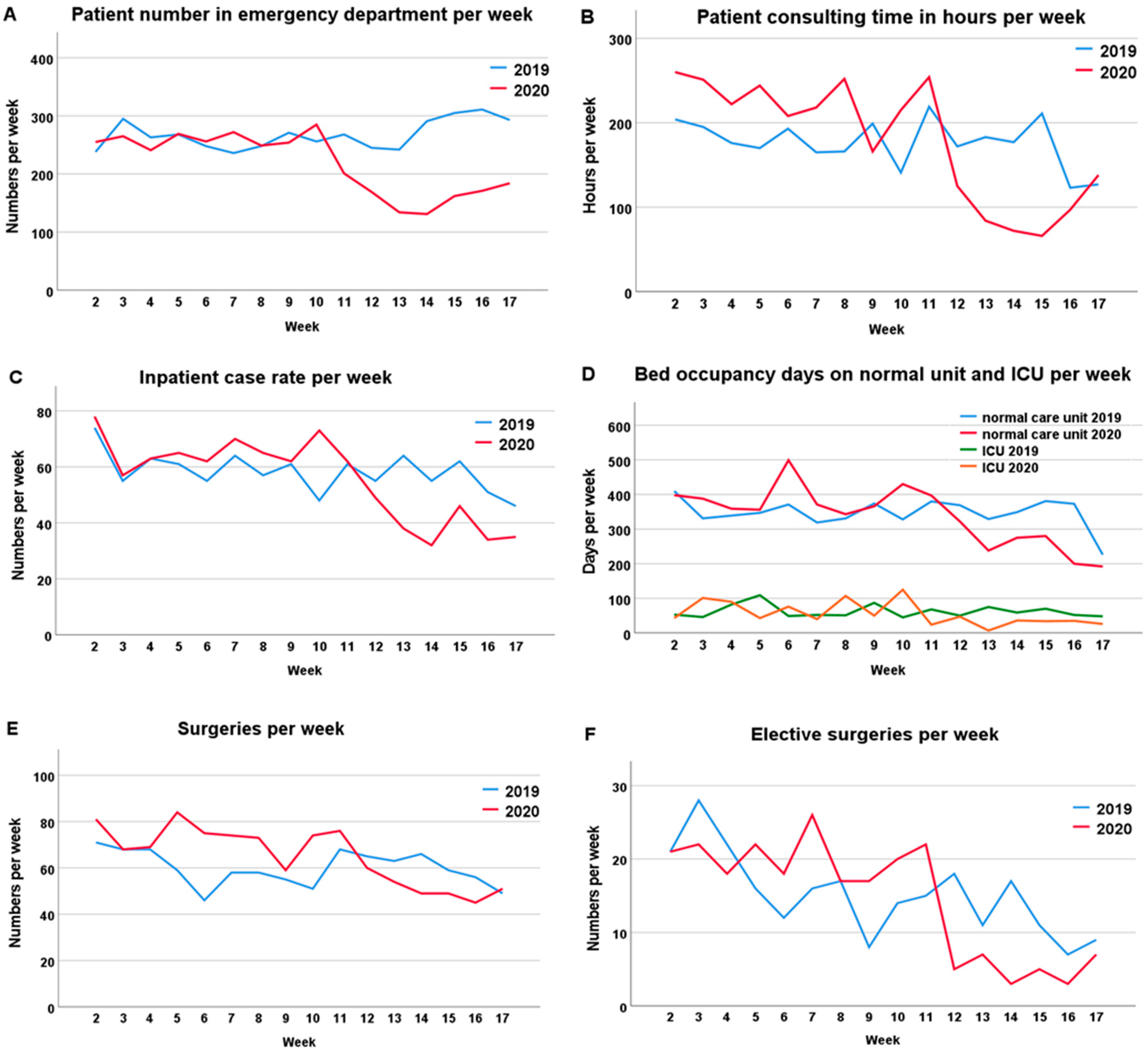
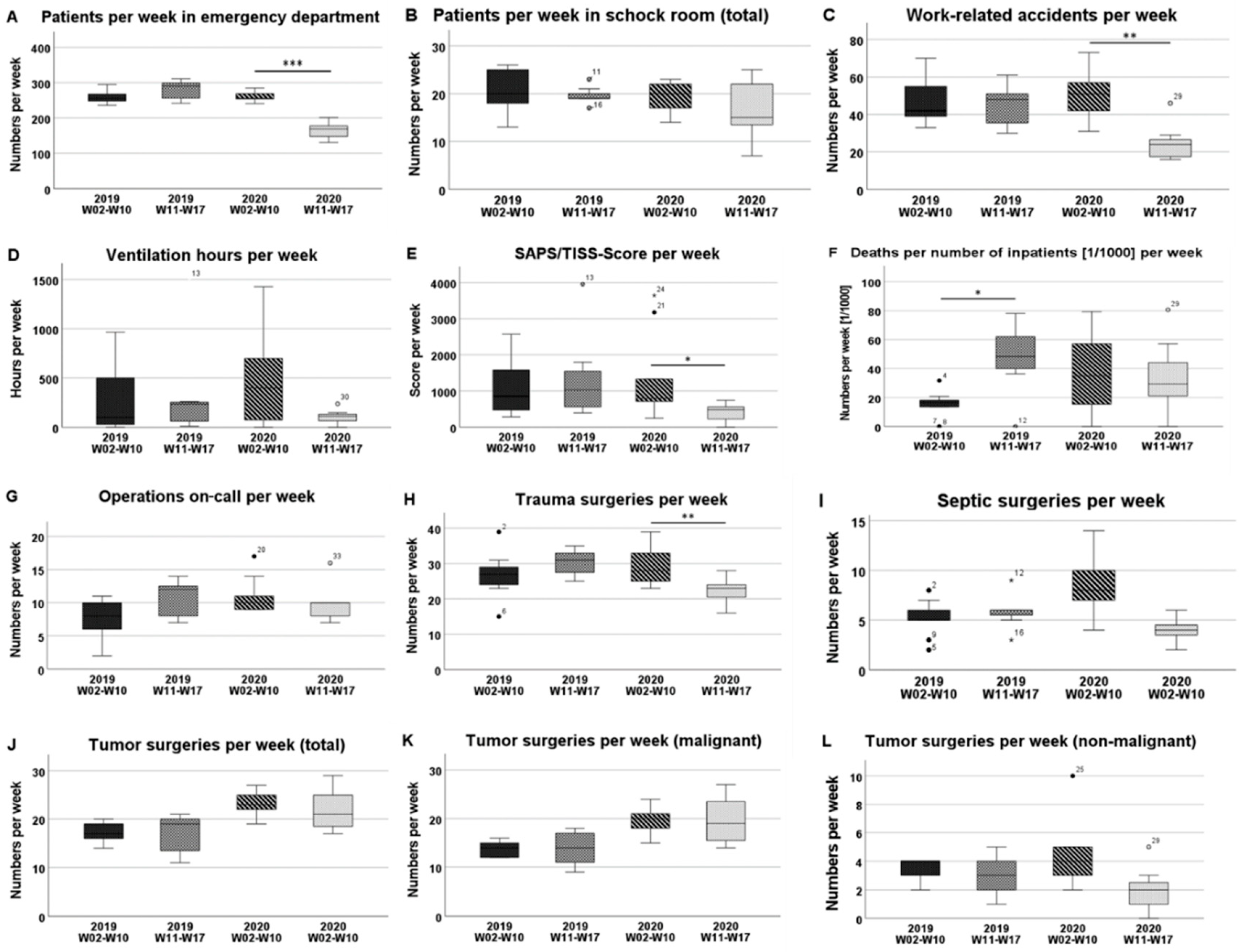
3.1. Emergency Department and Shock Room
3.2. Consulting Hours
3.3. Normal and Intensive Care Units
3.4. Operations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- USA Coronavirus Resource Center, John-Hopkins-University: Baltimore, Maryland, USA. Available online: https://coronavirus.jhu.edu/map.html (accessed on 18 November 2020).
- Bundesministerium für Gesundheit, Berlin, Germany. Available online: https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.html (accessed on 18 November 2020).
- Schädel-Höpfner, M. COVID-19—Eine Bewährungsprobe. Orthopädie Unf. 2020, 10, 66–67. [Google Scholar]
- Zaleski, A.T.; Taylor, B.A.; McKay, R.G.; Thompson, P.D. Declines in Acute Cardiovascular Emergencies during the COVID-19 Pandemic. Am. J. Cardiol. 2020, 129, 124–125. [Google Scholar] [CrossRef] [PubMed]
- Kansagra, A.P.; Goyal, M.S.; Hamilton, S.; Albers, G.W. Collateral Effect of Covid-19 on Stroke Evaluation in the United States. N. Engl. J. Med. 2020, 383, 400–401. [Google Scholar] [CrossRef] [PubMed]
- Garcia, S.; Albaghdadi, M.S.; Meraj, P.M.; Schmidt, C.; Garberich, R.; Jaffer, F.A.; Dixon, S.; Rade, J.J.; Tannenbaum, M.; Chambers, J.; et al. Reduction in ST-Segment Elevation Cardiac Catheterization Laboratory Activations in the United States During COVID-19 Pandemic. J. Am. Coll. Cardiol. 2020, 75, 2871–2872. [Google Scholar] [CrossRef] [PubMed]
- Sher, L. COVID-19, anxiety, sleep disturbances and suicide. Sleep Med. 2020, 70, 124. [Google Scholar] [CrossRef] [PubMed]
- Sher, L. An infectious disease pandemic and increased suicide risk. Braz. J. Psychiatry 2020, 42, 239–240. [Google Scholar] [CrossRef] [PubMed]
- The, L. The gendered dimensions of COVID-19. Lancet 2020, 395, 1168. [Google Scholar]
- Cluver, L.; Lachman, J.M.; Sherr, L.; Wessels, I.; Krug, E.; Rakotomalala, S.; Blight, S.; Hillis, S.; Bachman, G.; Green, O.; et al. Parenting in a time of COVID-19. Lancet 2020, 395, e64. [Google Scholar] [CrossRef]
- Campbell, A. An increasing risk of family violence during the Covid-19 pandemic: Strengthening community collaborations to save lives. Forensic Sci. Int. Rep. 2020, 2, 100089. [Google Scholar] [CrossRef]
- Thaler, M.; Khosravi, I.; Leithner, A.; Papagelopoulos, P.J.; Ruggieri, P. Impact of the COVID-19 pandemic on patients suffering from musculoskeletal tumours. Int. Orthop. 2020, 44, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Pichard, R.; Kopel, L.; Lejeune, Q.; Masmoudi, R.; Masmejean, E.H. Impact of the COronaVIrus Disease 2019 lockdown on hand and upper limb emergencies: Experience of a referred university trauma hand centre in Paris, France. Int. Orthop. 2020, 44, 1497–1501. [Google Scholar] [CrossRef] [PubMed]
- Houshyar, R.; Tran-Harding, K.; Glavis-Bloom, J.; Nguyentat, M.; Mongan, J.; Chahine, C.; Loehfelm, T.W.; Kohli, M.D.; Zaragoza, E.J.; Murphy, P.M.; et al. Effect of shelter-in-place on emergency department radiology volumes during the COVID-19 pandemic. Emerg. Radiol. 2020, 27, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Garude, K.; Natalwala, I.; Hughes, B.; West, C.; Bhat, W. Patterns of Adult and Paediatric Hand Trauma during the COVID-19 Lockdown. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1575–1592. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Li, X.; Wu, Y.; Xu, C.; Li, L.; Yang, J.; Fang, S. Community quarantine strategy against coronavirus disease 2019 in Anhui: An evaluation based on trauma center patients. Int. J. Infect Dis. 2020, 96, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Haffer, H.; Schomig, F.; Rickert, M.; Randau, T.; Raschke, M.; Wirtz, D.; Pumberger, M.; Perka, C. Impact of the COVID-19 Pandemic on Orthopaedic and Trauma Surgery in University Hospitals in Germany: Results of a Nationwide Survey. J. Bone Jt. Surg. Am. 2020, 102, e78. [Google Scholar] [CrossRef] [PubMed]
- Grassi, A.; Pizza, N.; Tedesco, D.; Zaffagnini, S. The COVID-19 outbreak in Italy: Perspectives from an orthopaedic hospital. Int. Orthop. 2020, 44, 1543–1547. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, R.; Edwards, S.; Kurihara, H.; Bass, G.A.; Balogh, Z.J.; Tilsed, J.; Faccincani, R.; Carlucci, M.; Martinez Casas, I.; Gaarder, C.; et al. European Society of Trauma and Emergency Surgery (ESTES) recommendations for trauma and emergency surgery preparation during times of COVID-19 infection. Eur. J. Trauma Emerg. Surg. 2020, 46, 505–510. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Numbers per Week | 2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|
| W02–W10 | W11–W17 | p-Value | ∆ (%) | W02–W10 | W11–W17 | p-Value | ∆ (%) | |
| Patients emergency department | 258 ± 19 | 279 ± 28 | 0.174 | 8 | 261 ± 13 | 165 ± 25 | <0.001 | −37 |
| (244; 272) | (253; 305) | (250; 271) | (141; 188) | |||||
| Shock room treatment | 20 ± 5 | 20 ± 2 | 0.758 | 0 | 19 ± 3 | 17 ± 6 | 0.470 | −11 |
| (17; 24) | (18; 21) | (17; 22) | (11; 23) | |||||
| Work-related accidents | 46 ± 12 | 45 ± 12 | 0.918 | −2 | 51 ± 12 | 25 ± 10 | 0.001 | −51 |
| (37; 55) | (34; 55) | (42; 61) | (15; 34) | |||||
| Patients in consultation hours | 179 ± 21 | 173 ± 37 | 1.000 | −3 | 226 ± 29 | 119 ± 65 | 0.012 | −47 |
| (163; 195) | (139; 208) | (204; 249) | (60; 180) | |||||
| Inpatient case numbers | 60 ± 7 | 56 ± 7 | 0.408 | −7 | 66 ± 7 | 42 ± 11 | 0.001 | −36 |
| (54; 65) | (50; 62) | (61; 71) | (32; 52) | |||||
| Mean hospital stay (days) | 7.2 ± 0.9 | 6.8 ± 0.6 | 0.252 | −6 | 7.7 ± 1.6 | 6.7 ± 1.9 | 0.114 | −13 |
| (7; 8) | (6; 7) | (6; 9) | (5; 9) | |||||
| Inpatient occupancy (days) (total) | 420 ± 39 | 421 ± 63 | 0.606 | 0 | 492 ± 63 | 308 ± 78 | <0.001 | −37 |
| (390; 450) | (362; 479) | (444; 541) | (236; 380) | |||||
| Inpatient occupancy (days) (normal care) | 350 ± 29 | 344 ± 55 | 0.606 | −2 | 390 ± 48 | 272 ± 72 | 0.005 | −30 |
| (327; 373) | (293; 395) | (353; 427) | (206; 338) | |||||
| Inpatient occupancy (days) (ICU) | 64 ± 23 | 60 ± 11 | 0.837 | −6 | 75 ± 32 | 30 ± 13 | 0.001 | −60 |
| (46; 81) | (50; 70) | (50; 100) | (18; 41) | |||||
| SAS/TISS-Score | 1148 ± 820 | 1371 ± 1242 | 0.758 | 19 | 1351 ± 1213 | 399 ± 281 | 0.023 | −70 |
| (517; 1778) | (223; 2520) | (419; 2283) | (139; 659) | |||||
| Ventilation hours | 292 ± 349 | 340 ± 523 | 0.981 | 16 | 455 ± 480 | 106 ± 78 | 0.210 | −77 |
| (24; 560) | (−144; 823) | (86; 824) | (34; 178) | |||||
| Deaths per inpatients (1/1000) | 15 ± 10 | 47 ± 25 | 0.012 | 213 | 36 ± 27 | 34 ± 27 | 1.000 | −9 |
| (7; 23) | (24; 70) | (15; 56) | (10; 59) | |||||
| Total number of surgeries | 59 ± 8 | 61 ± 7 | 0.758 | 3 | 73 ± 7 | 55 ± 10 | 0.012 | −25 |
| (53; 66) | (55; 67) | (67; 79) | (45; 65) | |||||
| Elective surgeries | 17 ± 6 | 13 ± 4 | 0.142 | −24 | 20 ± 3 | 7 ± 7 | 0.008 | −65 |
| (13; 22) | (9; 16) | (18; 22) | (1; 14) | |||||
| Operations on-call | 8 ± 3 | 11 ± 3 | 0.091 | 38 | 11 ± 3 | 10 ± 3 | 0.536 | −9 |
| (5; 10) | (8; 13) | (9; 13) | (7; 13) | |||||
| Tumor surgeries (total) | 17 ± 2 | 17 ± 4 | 0.918 | 0 | 24 ± 3 | 22 ± 5 | 0.408 | −8 |
| (16; 19) | (13; 21) | (22; 26) | (18; 26) | |||||
| Tumor surgeries (non-malignant) | 3.4 ± 0.9 | 3 ± 1.5 | 0.536 | −12 | 4.2 ± 2.4 | 2 ± 1.7 | 0.055 | −52 |
| (3; 4) | (2; 4) | (2; 6) | (0; 4) | |||||
| Tumor surgeries (malignant) | 14 ± 2 | 14 ± 4 | 0.837 | 0 | 19 ± 3 | 20 ± 5 | 1.000 | 5 |
| (13; 15) | (10; 17) | (17; 22) | (15; 24) | |||||
| Trauma surgeries | 27 ± 6 | 30 ± 4 | 0.174 | 11 | 30 ± 6 | 22 ± 4 | 0.008 | −27 |
| (22; 32) | (27; 34) | (25; 34) | (19; 26) | |||||
| Septic surgeries | 5 ± 2 | 6 ± 2 | 0.536 | −20 | 9 ± 3 | 4 ± 1 | 0.002 | −56 |
| (4; 7) | (4; 8) | (6; 11) | (3; 5) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polan, C.; Burggraf, M.; Kauther, M.D.; Meyer, H.-L.; Rademacher, F.; Braitsch, H.; Jöckel, K.-H.; Hardes, J.; Streitbürger, A.; Dudda, M. Development of Case Numbers during the COVID-19 Pandemic in a Center of Maximum-Care for Traumatology and Orthopedic Oncology. Healthcare 2021, 9, 3. https://doi.org/10.3390/healthcare9010003
Polan C, Burggraf M, Kauther MD, Meyer H-L, Rademacher F, Braitsch H, Jöckel K-H, Hardes J, Streitbürger A, Dudda M. Development of Case Numbers during the COVID-19 Pandemic in a Center of Maximum-Care for Traumatology and Orthopedic Oncology. Healthcare. 2021; 9(1):3. https://doi.org/10.3390/healthcare9010003
Chicago/Turabian StylePolan, Christina, Manuel Burggraf, Max Daniel Kauther, Heinz-Lothar Meyer, Friederike Rademacher, Henrik Braitsch, Karl-Heinz Jöckel, Jendrik Hardes, Arne Streitbürger, and Marcel Dudda. 2021. "Development of Case Numbers during the COVID-19 Pandemic in a Center of Maximum-Care for Traumatology and Orthopedic Oncology" Healthcare 9, no. 1: 3. https://doi.org/10.3390/healthcare9010003