Article Text

Abstract
Introduction Early non-pharmacological interventions can prevent cognitive decline in older adults with mild cognitive impairment (MCI). Creative expression (CrExp) can potentially mitigate cognitive decline and enhance the physical and mental health of older people. However, it is unclear whether activities involving CrExp can improve cognitive function and other health-related outcomes in older adults with MCI. The aim of the present study is to develop a Creative Expressive Arts-based Storytelling (CrEAS) programme that integrates verbal and non-verbal expressive activities and evaluate its effectiveness in improving cognitive function and other outcome indicators so as to explore its possible mechanism from the perspective of neuroimaging.
Methods and analysis This parallel randomised controlled trial with three arms (one intervention and two control arms) will be conducted over a 24-week period. A total of 111 participants will be enrolled and randomised to the CrEAS, recreation and usual activity groups. The CrEAS programme combines visual arts therapy and storytelling (TimeSlips) under the Expressive Therapy Continuum theoretical framework and provides an opportunity for people with MCI to actively engage in activities to improve cognitive function through verbal and nonverbal CrExp. Global cognitive function, specific domains of cognition (memory, executive function, language and attention) and other health-related outcomes (anxiety, depression and quality of life) will be measured at baseline, at the end of the intervention, and at the 24-week follow-up. Structural/functional brain MRI data will be collected at baseline and immediately after the intervention.
Ethics and dissemination Ethics approval was obtained from the Ethics Committee of Fujian Provincial Hospital (K2018-03-061). The study results will be disseminated through peer-reviewed journals and at academic conferences.
Trial registration number ChiCTR1900021526.
- clinical trials
- magnetic resonance imaging
- dementia
- neurology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a novel and innovative randomised controlled trial that will evaluate the effect of activities involving multiple integrated forms of creative expression on cognitive function and other outcome indicators in older people with mild cognitive impairment.
The study design includes two control groups for performance assessment to take into account ethical issues and bias from motivation and engagement.
The effectiveness of the intervention will be evaluated by multiple approaches including neuropsychological testing and resting-state MRI and is expected to reveal the mechanistic basis for the effect of the intervention on cognitive function and brain functional network connectivity.
This is a short-term exploratory study, and the results will require validation in a multicentre trial with a large sample size and longer follow-up period.
Introduction
Among individuals over the age of 65 years, the prevalence of dementia approximately doubles every 4 or 5 years; thus, dementia occurs in more than one-third of individuals over 85 years old.1 2 In 2018, 50 million people worldwide were living with dementia, and it is estimated that the number will exceed 152 million by 2050.3 China has the largest population of patients with dementia in the world, and the incidence of dementia among people over 60 years old is predicted to increase from 14% by 2015 to a staggering 33% by 2050, imposing a heavy social and economic burden on individuals, families, communities and the country as a whole.2 4 5
Given that dementia is non-curable and irreversible, increasing attention has been paid to its prevention. Mild cognitive impairment (MCI)—a neurological disorder between normal function and dementia4—is a key stage at which dementia may be delayed or prevented through early intervention.6 One-fifth of the population over 65 years of age is affected by MCI and may benefit from targeted interventions.7 Indeed, several trials involving older adults with MCI are currently underway that are testing different pharmacological and non-pharmacological strategies to delay the onset of cognitive decline, for which there are currently no effective treatments.8 There is evidence that non-pharmacological interventions improve cognitive functioning in older adults with MCI4 8 but not all have demonstrated clinical benefits, thus highlighting the need for more effective or creative approaches. Clinical trials provide an opportunity for interested persons to receive new treatments, which is particularly important when no pharmacological options are available.8
Creative expression (CrExp) is characterised by the production of novel or original objects, ideas, perspectives or processes.9 For individuals with cognitive impairment, CrExp offers an opportunity for self-expression, social interaction, communication, sensory stimulation and emotional relief in a failure-free setting.9 CrExp activities such as storytelling, visual arts, dance, music and dramatic arts are innovative, non-pharmacological interventions that have been applied in clinical settings involving children, patients with cancer, older people and patients with MCI and dementia.10–15 Among the different types of CrExp, visual arts may be especially useful for people with normal or suboptimal cognition as they have been shown to improve cognitive function, psychological symptoms, physiological state, social well-being and connectedness in older adults with or without cognitive dysfunction,13 16–21 although the findings in individuals exhibiting cognitive decline are controversial. A systematic review of the literature revealed that visual arts therapy has a positive effect on depression, anxiety, quality of life (QoL), coping ability and self-esteem but has no clinically significant effect on cognition.22 On the other hand, a combination of art-based activities and other therapies (eg, physical exercise, cognitive stimulation, music and horticultural therapies) was shown to result in cognitive improvement.23 24 Visual art therapy may enhance cognition in a wide range of individuals but may be particularly effective in those at high risk for dementia.25 26 However, there are many unanswered questions and methodological issues in studies assessing the efficacy of art-based therapy on cognition in older adults experiencing cognitive decline.
Our earlier work in a randomised controlled trial (RCT) comparing the effects of standard cognitive training with a CrExp programme for older people with MCI found that the latter had beneficial effects on cognitive function and daily living ability.13 A subsequent exploratory RCT examining the efficacy of CrExp therapy (with the control group receiving standard cognitive training) in older people with dementia demonstrated significant improvements in cognitive function, QoL, level of depression, communication ability and emotional status.27 The main form of CrExp activities in these two studies was storytelling. The TimeSlips storytelling initiative, which was developed in the 1990s for use with persons affected by dementia of varying severity, employs visual images to encourage spontaneous, improvisational responses, which provides participants with a sense of uniqueness, belonging, support and value while eliciting pleasure and other positive emotions.28–30 Storytelling is an important way to communicate and share ideas, life experiences and insights into different topics and provides an opportunity to connect with others.31
Art activities and storytelling have each been incorporated into therapeutic approaches for older adults with cognitive impairment. However, their combination may be more beneficial to mental health than each activity alone. Visual art therapy provides psychological benefits and improves cognitive function by allowing self-expression through non-verbal communication,20 while the storytelling encourages social interaction through verbal communication, which assigns the storyteller a valuable social role that can enhance their sense of well-being.27 32 Combining these interventions can have synergistic effects.
Although CrExp activities have received greater support from the medical and scientific communities over the past few years as a viable treatment option for cognitive impairment in older adults, the neural mechanisms underlying the observed cognitive changes are not well understood. A functional brain network is established through neural connections between various regions of the brain; the degree of correlation between neural signals reflects the strength of the functional connections in corresponding regions and hence, short-term functional changes in the brain. Brain functional network analysis thus provides a means of investigating the mechanistic basis for the effects of short-term cognitive interventions. Studies have shown that visual creativity can activate and enhance functional interregional connectivity in the brain.33 34
CrExp activities are thought to exert cognitive benefits by stimulating the central nervous system through engagement in tasks involving creativity, abstract thinking, planning, different forms of expression and cognitive control; this effect is likely mediated through increased functional connectivity in the brain.
We aimed to develop a Creative Expressive Arts-based Storytelling (CrEAS) programme and conduct a methodologically rigorous RCT to evaluate its effects on neuropsychological outcomes in older adults with MCI. Participants will undergo structural and functional MRI (sMRI and fMRI, respectively) before and after the intervention to examine the neural basis for the effects of the intervention. The study design includes active and waitlist control groups to take into account ethical issues and bias from motivation and engagement. In other studies, the intervention period of art-based activities for older people or for those with cognitive impairment ranged from 3 to 40 weeks, with no consensus as to the optimal duration.17 35–37 Based on the results of our previous work,13 we determined that an intervention cycle of 24 weeks and frequency of once a week can achieve clinical benefits. We hypothesise that the 24-week CrEAS intervention will result in greater improvement in cognitive function and other health-related outcomes in older adults with MCI compared with those who continue their usual activities or receive other types of recreational intervention, and that this will be accompanied by favourable changes in functional connectivity of specific brain regions.
Methods and analysis
Study design and registration
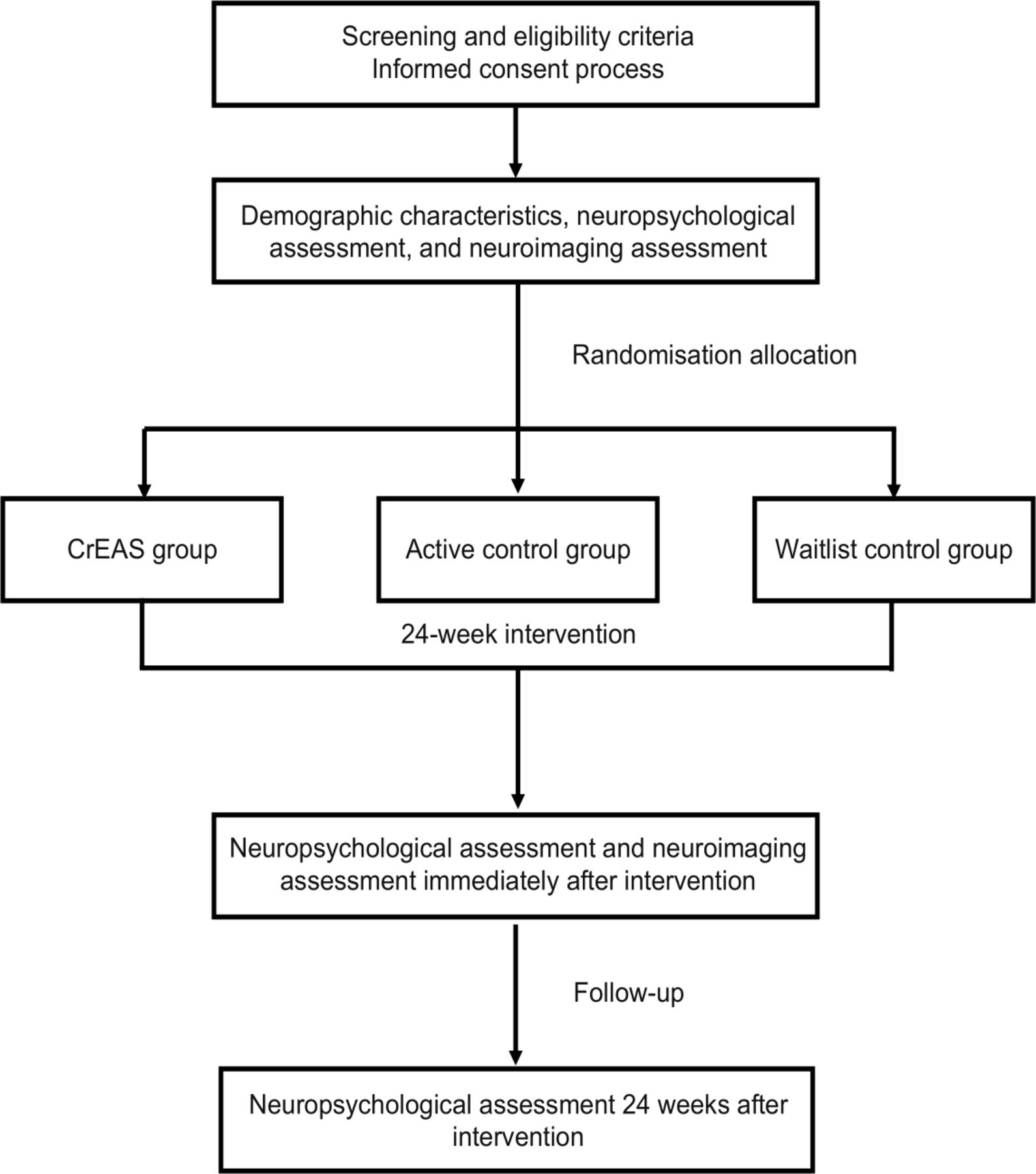
The study design is an RCT with three parallel groups in a 1:1:1 allocation ratio, with allocation concealment and assessor blinding. The trial will be conducted in accordance with the Standard Protocol Items for Randomised Trials and Consolidated Standards of Reporting Trials guidelines for non-pharmacological interventions (figure 1).38 Individuals with MCI will be recruited from two centres—namely, Fujian Provincial Hospital and Fujian Provincial Hospital South Branch. A total of 111 eligible participants will be randomised to the 24-week CrEAS intervention (90 min per session, once a week), 24-week recreation intervention (90 min per session, once a week) or 24-week waitlist control group. Global cognitive function and specific domains of cognition (memory, processing speed, executive function, attention and verbal learning and memory) as well as other health-related outcomes will be assessed at baseline before randomisation and at the end of the intervention, while the structure and function of brain regions related to cognition will be assessed by fMRI at these time points.

Flow diagram of the study design.
Recruitment of participants started in December 2019 and the study will be completed in June 2021. All participants will be provided with consent forms. The trial is registered in the Chinese Clinical Trials Registry.
Participants
Recruitment and screening
The following strategies will be used to ensure adequate enrolment and reach the target sample size: (1) targeted recruitment through memory clinics and the neurology department of the participating hospitals, (2) study posters with the contact information of the researchers posted on notice boards of the participating hospitals, (3) health seminars held at the hospitals’ health promotion centres and (4) word-of-mouth by the researchers.
Interested individuals will be instructed on how they can participate in the trial through telephone calls or visits to the participating hospitals. Potential participants who respond to the recruitment strategies and contact the researchers will be screened for study eligibility and safety in a two-stage process consisting of phone and in-person interviews.
Phone interview: the study staff will obtain verbal consent from the respondent for their participation in the phone and in-person screenings as well as the respondent’s self-reported health history. Potential participants who pass the phone screening will be scheduled for an in-person interview to screen for eligibility.
In-person interview: the study staff will corroborate the information obtained during the phone screening, perform an assessment for MCI and complete the MRI safety check. Participants who meet the following inclusion and exclusion criteria will be enrolled. The clinical research coordinator will explain the study to the participants, who will be asked to voluntarily sign an informed consent form before participation.
Inclusion criteria
Participants must meet the following Peterson diagnostic criteria for MCI39: (1) memory problems, preferably confirmed by an informant, (2) memory impairment in accordance with age and education level (Montreal Cognitive Assessment (MoCA) score of 13/14 for individuals with no formal education, 19/20 for individuals with 1–6 years of education and 24/25 for individuals with ≥7 years of education), (3) preserved general cognitive function (Mini-Mental State Examination score between 24 and 30), (4) intact activities of daily living (ADL) (Lawton–Brody ADL score <18) and (5) absence of dementia. The final clinical diagnosis will be made by experienced psychiatrists according to the Diagnostic Statistical Manual of Mental Disorder, Fourth Edition criteria for MCI. Eligible participants must meet the following criteria: (1) diagnosis of MCI, (2) age 60–85 years inclusive, (3) visual and auditory acuity adequate for neuropsychological testing and (4) willingness to provide informed consent.
Exclusion criteria
Exclusion criteria were as follows: (1) severe aphasia or other factors that could preclude completion of neuropsychological assessment or the CrEAS programme, (2) gastrointestinal, renal, hepatic, respiratory or other systemic diseases, (3) other disorders or use of medication that could affect cognitive functions, (4) neurological or psychiatric conditions that could affect cognition (eg, Parkinson’s disease, stroke, schizophrenia), (5) participation in another clinical study and (6) contraindication for MRI (only for the MRI examination).
Withdrawal criteria
Participants will be allowed or required to withdraw from the trial based on the following: (1) unwillingness to continue participating, (2) adverse events such as severe illness during the intervention and (3) taking drugs or receiving other cognitive or professional treatment during the study.
Sample size determination
Sample size was calculated based on an improvement in MoCA scores. Similar RCTs13 using CrExp therapy for older adults with MCI showed effect sizes for MoCA scores of 24.68±1.84 (intervention group) and 23.13±1.68 (control group). A sample size of 29 participants per group was determined as being sufficient to detect an effect with a type 1 error rate of 5% (α=0.05) and 90% power (β=0.10) using PASS V.11.0 software (NCSS, Kaysville, Utah, USA). Taking into consideration a 20% attrition rate, a total of 111 participants was needed, with 37 participants per group.
Randomisation, allocation concealment and blinding
Participants will be randomised (after obtaining written, informed consent; screening and obtaining baseline measurements) to the CrEAS, active control or waitlist control group at a 1:1:1 ratio. Before randomisation, a researcher not involved in subject recruitment and data collection will prepare a randomisation list with 37 sets of numbers, where 1, 2 and 3 represent the CrEAS, active control and waitlist control groups, respectively, using Research Randomizer software (http://www.randomizer.org/). These 37 sets of 111 numbers will be separately printed and each will be sealed in an envelope. After subject recruitment, the researcher will randomly select an envelope to confirm group assignment. Due to the nature of non-pharmacological interventions, the data collector and statisticians—but not the participants and intervention staff—will be blinded.
Intervention
Intervention group
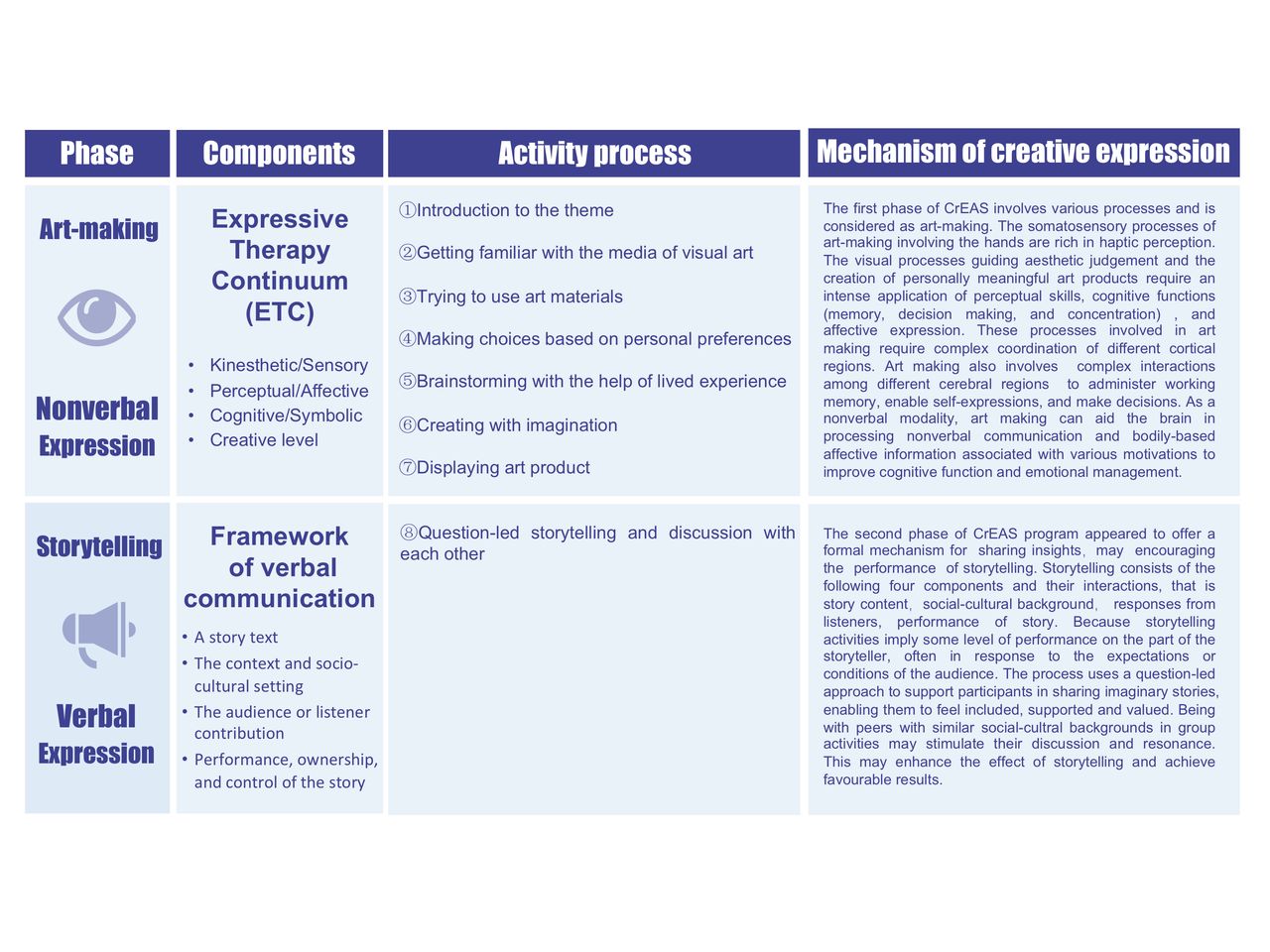
The CrEAS programme is a new non-pharmacological intervention that combines visual arts therapy with storytelling (TimeSlips) under the Expressive Therapy Continuum (ETC) theoretical framework.40 The programme provides an opportunity for participants to actively engage in activities that improve cognitive function through verbal and nonverbal CrExp. In accordance with the Medical Research Council (MRC) guidance for the development and evaluation of complex interventions,41 42 the programme was pretested in terms of feasibility in a pilot study. There were two main stages in the design of the CrEAS programme model that guided the development of the programme of activities based on ETC and storytelling components (figure 2). Participants in the CrEAS group will engage in CrExp activities for 24 weeks at a frequency of once per week and 90 min per session, including 60 min of art-making and 30 min of storytelling, under the guidance of an accredited instructor and two auxiliary staff members. The detailed content of the CrEAS programme is shown in table 1.
CrEAS programme
{kind=link}
{kind=link}
The CrEAS programme model. The model will serve as a guide for the targeted interventions in this study; theoretical elements will be used as the basis for formulating an activity plan and for explaining the possible mechanisms underlying the effects of CrExp activities. CrEAS, Creative Expressive Arts-based Storytelling; CrExp, creative expression.
The ETC is a theoretical model for the assessment and application of media in art therapy.43 It can be used to evaluate the predominance of sensory information processing based on the configuration of formal elements in the artwork and the interaction of the art-maker with the materials. The model also accounts for the effects of the texture and fluidity of the art materials, which are thought to differentially affect cognitive processing and to differ in their potential to elicit emotion.44 Based on the ETC, various techniques such as drawing, collage, painting, clay work, origami and quilling will be used in the art-making. The materials used will include but will not be limited to pencils, colour pens, crayons, pastels, watercolour paints and paper. Each session will have a preplanned theme and prepared materials. The CrEAS protocol is detailed in online supplemental file 1.
Supplemental material
For storytelling, participants will form a circle and a facilitator will prompt the group with a series of open-ended questions (who, what, where, when, how and why) in reference to artwork completed in the art-making stage, with the aim of eliciting an imaginative response. Participants will be encouraged to share their artwork with the group and vocalise any thought that comes to mind. Responses are woven into an inclusive narrative by the facilitator that is periodically read back to the participants to help them further develop the story or bring it to a conclusion.
Active control group
Participants in the active control group will participate once a week for 24 weeks in group recreational activities facilitated by geriatric nurses. Arts interventions are frequently criticised for lacking a comparator group, which limits the inferences that can be drawn regarding the importance or necessity of the art component45; that is, the benefits derived from these interventions have been attributed to social interactions alone.46 In this study, non-art-focused social activities will be designed to allow comparisons with the intervention group; these will consist of a 15 min interaction game as a warm-up session, followed by 75 min of puzzle games such as Magic Square, Jigsaw, Unblock Me, Tangram and Sudoku, among others. No specific CrExp activity will be administered to the control group.
Waitlist control group
Participants in the waitlist control group will engage in their usual activities during the 24 weeks following baseline assessment. After the study, if the other two groups show significant improvements in cognitive function, participants in the waitlist control group will be offered the relevant intervention as a courtesy for their participation.
Study settings
Screening and non-imaging data collection will be performed at the memory clinics of Fujian Provincial Hospital and Fujian Provincial Hospital South Branch. Imaging data will be obtained at the Centre for Magnetic Resonance Research of Fujian Provincial Hospital. The CrEAS programme (intervention group) will be implemented and recreational activities (active control group) will be performed at the Centre for Health Education and Health Promotion at the two hospitals.
Outcome measures
Demographic characteristics (eg, age, sex, marital status, education level, occupation and socioeconomic status) and history of disease and medication use will be recorded during the initial evaluation. Participants will be assessed before, immediately after and 24 weeks after the intervention. Outcome measures will include neuropsychological and neuroimaging parameters. All assessments included in the trial are shown in table 2.
Assessment outline and timelines
Neuropsychological assessment
Various measurements will be obtained to evaluate the effects of the intervention. Outcome measures other than cognitive function will be selected based on the previous studies of art-based interventions in MCI and Alzheimer’s disease that reported statistically significant improvements in psychological well-being20 47 48 and QoL.18 22 49 In the present study, the neuropsychological evaluation will include several commonly used measures of cognitive function, functional status, psychological well-being and QoL.
Primary outcome
The MoCA is a brief but reliable test that evaluates visuospatial/executive function, naming, memory, attention, language, abstraction, delayed recall and orientation.50 The Changsha MoCA (MoCA-CS) is the Chinese version of the MoCA that was modified from the original (English) version based on Chinese cultural, linguistic and population characteristics. Scores range from 0 to 30, with a lower score indicating lower cognition function.50 The primary outcome (global cognitive function) will be measured with the MoCA-CS, which is widely used in China and has good reliability and validity.51 52
Secondary outcomes
Memory function will be assessed using the Auditory Verbal Learning Test,53 which adopts the rationale and methods of the California Verbal Learning Test and Hong Kong Verbal Learning Tests. The word list consists of 12 two-character words from three semantic categories (flowers, occupations and apparels), with four words in each category. The indicators are immediate recall, delayed recall (after a delay of 20 min, during which a non-verbal task is performed) and recognition (12 target words and 12 semantically related distractor words).
Executive function will be evaluated with the Shape Trail Test (STT), a culture-neutral variant of the Trail Making Test that minimises cultural bias and provides a more accurate cognitive measure of Chinese subjects.54 The STT-A requires subjects to connect numbers from 1 to 25; the STT-B shows all numbers (from 1 to 25) two times, once in a circle and once in a square, and subjects are required to draw alternating lines between the circles and squares.
Visuospatial construction ability will be measured with the widely used Rey-Osterrieth Complex Figure Test (ROCF).55 The three components of the test are copy, immediate recall and delayed recall. Subjects are given an ROCF stimulus card and asked to draw the same figure. They are then instructed to draw what they remember and after a delay of 30 min, they are required to redraw the same figure.
Language will be measured with the verbal fluency test and Boston Naming Test (BNT). The former requires subjects to list as many words as possible in a given semantic category (eg, animal) in 1 min.56 The Chinese version of the BNT, which has good validity and sensitivity,57 requires subjects to name 30 drawings that are presented to them.
Attention will be measured with the standardised Symbol Digit Modalities Test, which evaluates directed attention in a complex task.58 It requires subjects to substitute 10 geometric symbols that are presented to them with numbers from 1 to 10; the score is the correct number of substitutions in 90 s.
Anxiety will be measured with the Zung Self-Rating Anxiety Scale, a 20-item self-report assessment on a four-point scale from 1 (seldom) to 4 (most of the time), with total scores ranging from 20 to 80 and scores over 50 indicating mild to moderate anxiety.59
Depression will be evaluated with the Geriatric Depression Scale, a 30-item self-report assessment in which questions are answered with yes or no, with a score greater than 10 indicating depressive symptoms.60
QoL will be measured with the 13-item self-rated QoL in Alzheimer’s Disease scale, which has poor, fair, good and excellent as response options.61 Scores for each item range between 1 and 4 and total scores are between 13 and 52, with higher scores indicating a higher QoL.
Neuroimaging assessment
MRI scans will be acquired at baseline and a 24 weeks postintervention on a 3.0 T Prisma scanner (Siemens, Erlangen, Germany). Quality control checks on the phantom and imaging sequences will be performed before data collection. High-resolution T1-weighted images of the whole brain will be obtained using a sagittal 3D magnetisation-prepared rapid gradient echo sequence. Resting-state fMRI will be performed using a multiband echo-planar imaging sequence.
Data collection and analysis
Enrolled subjects will be scheduled to complete baseline data collection. Data will also be collected after 24 and 48 weeks (6-month follow-up) for cognition and other outcomes. During data collection, rest periods and snacks will be provided to participants as needed. sMRI and fMRI data will be collected at baseline and immediately after the intervention. Subjects who undergo MRI at baseline will be reevaluated for MRI eligibility at 24 weeks. To ensure that data collectors are blinded to group assignment, they will not interact with the subjects except during data collection.
To minimise selection bias, data will be analysed according to the intention-to-treat principle.62 Demographic and other baseline characteristics will be summarised with descriptive statistics. We will compare changes in neuropsychological test scores and other outcomes from baseline to 24 weeks and from baseline to 48 weeks for the three groups using a repeated-measures mixed linear model, which will be adjusted for potential confounders such as age, sex and education level. This analysis will be two-tailed with alpha level set at 0.05 and will be performed using SPSS V.21.0 software (IBM, Armonk, New York, USA). Missing data will be handled by multiple imputation.
sMRI, fluid-attenuated inversion recovery and blood oxygen level-dependent fMRI data will be collected in a 30 min session. High-resolution T1-weighted images of the whole brain will be obtained using a sagittal 3D magnetisation prepared rapid gradient echo sequence with the following parameters: repetition time (TR)=2530 ms; echo time (TE)=2.98 ms; slice thickness=1 mm; 192 slices; flip angle=7°; voxel size=1.0×1.0×1.0 mm3; field of view (FOV)=256×256 mm2. Resting-state fMRI will be conducted using a multiband echo-planar imaging sequence with the following parameters: TR=2000 ms; TE=30 ms; 33 slices; voxel-size=3.5×3.5×3.5 mm3; flip angle=90°; FOV=224×224 mm2. fMRI data will be processed using SPM V.12 (https://www.fil.ion.ucl.ac.uk/spm/software/spm12/) in MATLAB 2013b (MathWorks, Natick, Massachusetts, USA). fMRI data preprocessing will consist of slice-timing correction, realignment, coregistration, segmentation, spatial normalisation, Gaussian spatial smoothing, time series linear detrending, filtering and nuisance regression performed with 24 subject-specific realignment parameters; the signal from white matter and cerebrospinal fluid and their first-order derivatives will be included as confounds.
Data monitoring and interim analyses
The principal investigator will be responsible for reviewing the data in collaboration with the statisticians and ensuring their completeness and validity. Participants’ attendance and withdrawal rates, adherence and adverse events will be recorded in detail by the study coordinators, who will also ensure data creation, integrity, quality control checks and audits and will review the accuracy and completeness of data collection forms before the data are entered it into the hospital’s electronic information database.
Patient and public involvement
When designing the procedures, some experts will be invited to follow the development process of complex interventions in strict accordance with the MRC framework. Additionally, consumers will be invited to consult on the content of the CrEAS programme. Participants will not be involved in research design, recruitment, study execution or dissemination of study findings. We will use a satisfaction questionnaire and suggestion form to examine participants’ attitudes regarding this trial and obtain feedback.
Ethics and dissemination
This study strictly adheres to ethical principles outlined in the Declaration of Helsinki and respects the wishes of each participant. The protocol was approved by the Ethics Committee of Fujian Provincial Hospital (K2018-03-061). Before the study is initiated, the purpose, content and process of the study will be fully explained to each participant and written, informed consent will be obtained prior to their enrolment. The researchers will not release the subjects’ personal information or compromise their privacy under any circumstances. There are no plans to share the results of the study or details of the analysis of study data with the participants, which will be specified in the consent form. Cognitive test results and clinical diagnosis based on MRI scans will be provided on request to participants by the physician. Study results will be disseminated through peer-reviewed journals and at domestic and international academic conferences.
Discussion
Early non-pharmacological intervention is the mainstay of treatment for prevention and management of cognitive decline. Some studies have shown that participation in CrExp activities such as visual arts and storytelling can improve mental and physical health in older adults with cognitive impairment,16 63 64 although this remains controversial.37 We designed a CrEAS programme that integrates activities involving verbal and non-verbal expression and evaluated its effectiveness in improving cognitive function and other health-related outcomes in older adults with MCI. We will adopt rigorous methods to reduce bias such as randomisation, blinding, theoretical innovation and comparisons to a control group. The effectiveness of the intervention will be evaluated using different methods including neuropsychological testing and resting-state MRI; the latter is expected to provide insight into the neural mechanisms underlying the effects of the CrEAS programme. Another novel aspect of this trial is that it will compare the effects of CrExp versus standard recreational therapies on cognitive function.
This study has several limitations. First, there will be an unavoidable bias in participant selection as the older adults with MCI who are enrolled in the trial will tend to be highly motivated. Second, given the nature of non-pharmacological interventions, it is difficult to blind researchers and participants to group assignment. In addition, although we will use multiple strategies for subject recruitment, it will be difficult to ensure that eligible participants have not previously met or interacted. Distortion of the intervention will be difficult to control even if we explain its purpose and trial requirements in detail to the participants beforehand. Finally, because of planning constraints, we may need to perform postintervention assessment at a different time of day than the baseline assessment.
In conclusion, this trial will test whether CrExp in multiple forms can improve cognitive function in older adults with MCI. If the intervention is found to be effective, the results of this study will provide evidence that non-pharmacological therapy is effective for cognitive rehabilitation and potentially for preventing the progression of MCI to dementia.
Acknowledgments
The authors would like to thank the experts for their insightful advice, and thank the participants of this study and patient advisers for their support. The authors would also like to thank the staffs and management involved in the study at all the participating memory clinics.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RL and Y-JY are joint first authors. RL and Y-JY designed the study and drafted the manuscript. HL conceived the study, critically revised the manuscript, obtained funding and will supervise the study. YZ is in charge of coordination and direct implementation. Y-TL, Z-ZC and K-YZ helped to develop the study measures and analyses. All authors contributed to drafting the manuscript and have read and approved the final manuscript.
Funding This study was funded by the National Natural Science Foundation of China (81571379); Startup Fund for Scientific Research, Fujian Medical University, China (2018QH2023); and high-level hospital foster grants from Fujian Provincial Hospital, Fujian Province, China (2019HSJJ10).
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.