





Abstract
To estimate the impact of delays in surgery for hip fracture on short- and long-term outcomes.
Analysis of inpatient hospital data integrated with national health plan data and Central Bureau Statistics.
Seven major tertiary hospitals.
All consecutive elderly patients admitted with hip fracture during the years 2001–2005.
Time from the hospitalization to operation; one-year mortality.
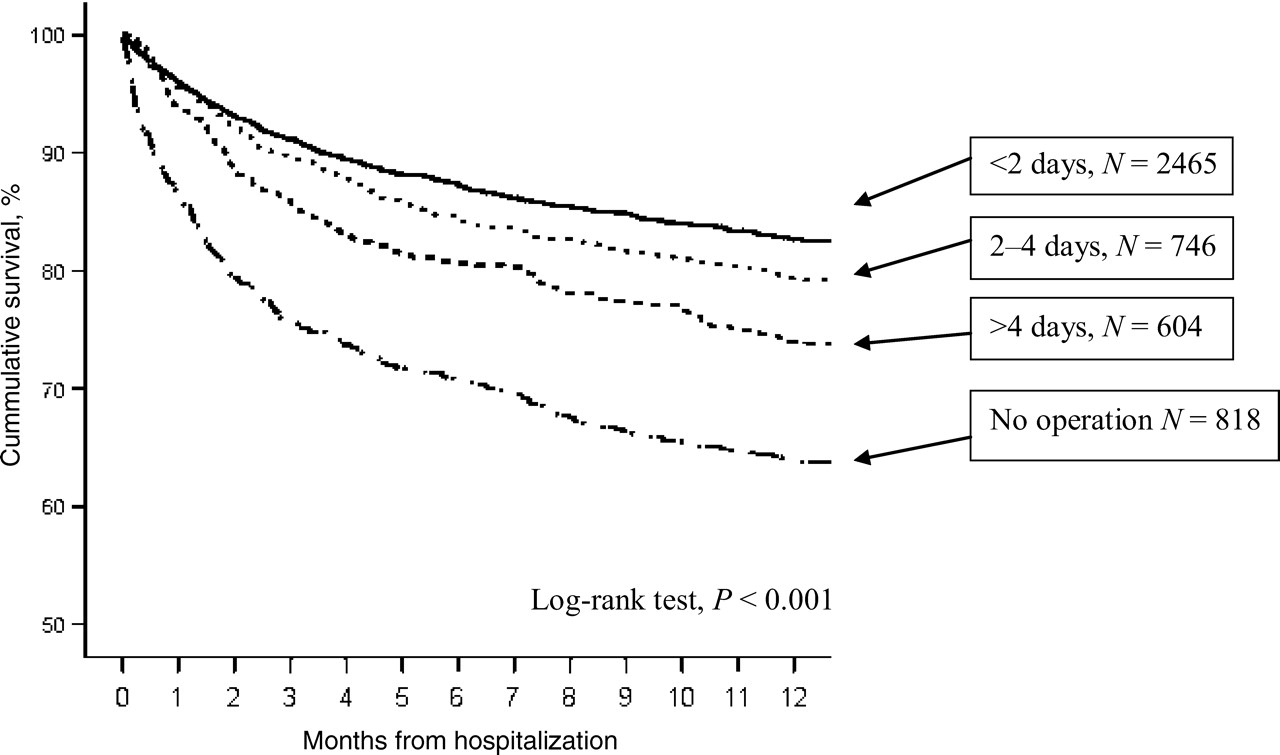
Study population comprise 4633 patients, older than 65 years. The conservative approach was chosen in 818 patients (17.7%), while 1350 patients (29.1%) waited >2 days from admission to the surgery. There was a substantial variation in median pre-operative stay among the hospitals (range 0–4 days). Patients who had surgery within 2 days had lower mortality (in-hospital, 1-month and 1-year) compared to those who waited for surgery >4 days (2.9%, 4.0%, 17.4% vs. 4.6%, 6.1%, 26.2%, respectively). A Cox proportional regression model of 1-year mortality in operated patients adjusted for background morbidity (Charlson index) showed that the length of operation delay has a gradual effect on increasing mortality (<2 days—reference group, 2–4 days—OR = 1.20, 5 days or longer, OR = 1.50). The 818 (17.7%) non-operated patients suffered the highest 1-year mortality, 36.2%.
Delays in surgery for hip fracture are associated with significant increase in short-term and 1-year mortality. Variation among the hospitals was substantial and calls for prompt quality improvement actions.
As the population ages, hip fractures in the elderly are becoming a growing medical and a social concern. There are estimates that the lifetime incidence of hip fractures is 18% in women and 6% in men, the 1-year case fatality approaches 20% and many survivors will need long-term care [1].
Whether early surgery is beneficial is a long-standing controversy and a frequent clinical concern in the acute management of patients with hip fracture. A randomized trial of surgical timing in hip fracture has never been attempted (and probably is not ethical to conceive). Various studies, mostly observational, reported that early surgery is associated with lower mortality, shorter length of hospitalization and lower rate of complications [2–8]. Many studies did not adjust for comorbidity or other parameters that might be used to ‘select’ patients for earlier surgery. Other studies that controlled for comorbidity did not find an association between late surgery (after 24–48 h) and increased mortality [9, 10]. Recently, the (Organization for Economic Co-operation and Development OECD) has included a 48-h waiting time to surgery in elderly patients with hip fracture in its national quality indicator list [11]. Others like the British Royal College of Physicians' guidelines recommend that patients should be operated on within 24 h of admission [12].
There is a need to confirm these observations and validate the guidelines in different health care systems. The primary purpose of this study, using an integrative database from Israel's largest health plan, was to examine the association between delays in surgery and short- and 1-year survival in elderly patients admitted with hip fractures. Furthermore, we evaluated inter-hospital variability, patient characteristics, management parameters and mortality outcomes.
Methods
Data on diagnoses, comorbid conditions, in-hospital management and outcome were taken from a central data warehouse of the Clalit Health Services, a non-governmental, not for-profit health maintenance organization which owns hospitals. National data on survival were obtained from the Central Bureau of Statistics. These data are relatively complete and are constantly updated by the Central Bureau of Statistics.
Seven large, general hospitals of Clalit Health Services organization throughout Israel were included in the study. These hospitals admit about one-third of all hip fracture cases in Israel. We screened all first admissions of the patients older than 65 years with primary diagnosis of fracture at the neck of femur (ICD-9-CM codes 820.X) between February 2001 and April 2005. Cases admitted after motor vehicle accidents were excluded.
We used the Charlson index to compute the burden of comorbid conditions [13]. The overall comorbidity score reflects the cumulative increased likelihood of 1-year mortality; the higher the score, the more severe the burden of comorbidity.
Five types of operation for hip fracture were identified (ICD-9-CM procedures codes): closed reduction of fracture of femur with internal fixation (Z79.15); Knowles nailing—close reduction of fracture of femur neck (Z79.150); open reduction of fracture of femur with internal fixation (Z79.35), Richard's hip nailing (Z79.350) and joint replacement of lower extremity (arthroplasty, Z81.5).
Time to surgery was defined as the number of calendar days between admission and surgery and grouped as follows: <2, 2–4 and >4 days. Total length of stay and stay after surgery were similarly calculated. For each patient we used the following outcome measures: in-hospital, 1-month and 1-year mortality from any cause, and any emergency readmission within 30 days of initial admission.
Statistical analysis
For univariate analysis, we used t-test and ANOVA test for comparison of continuous variables and Pearson's chi-square test for categorical variables. Normality of the data was tested with a one-sample Kolmogorov–Smirnov test to indicate the appropriateness of parametric testing. Mann–Whitney test and Kruskal–Wallis tests were used for comparison of variables with not normal distribution. All variables found to be related to the survival time with the level of P-value <0.1 were included in the multivariate analysis. For evaluating 1-year survival time, Cox regression models were used. We stratified the patients into four groups band on age: <70, 70–80, 80–90 and >90 years. Comorbidity conditions were included first as separate diagnoses (ischemic heart disease, chronic obstructive pulmonary disease, dementia, diabetes, arterial hypertension, hypothyroidism) and second as comorbidity index (Charlson). Operation delay time was stratified into four groups as follows: <2, 2–4, >4 days and not operated patients. Patients' group operated within less than 2 days served as a reference group. In Cox regression model, we reported all variables found to be significant with level of <0.10.
For evaluating hospital-adjusted variations in 1-year mortality, we built a Cox regression model using the hospital with the lowest 1-year mortality as a reference group.
For assessing the association between surgery delay time and post-operative length of the hospitalization, linear regression model was built. Since post-operative length of stay did not distribute normally, transformation by natural logarithm was performed.
All reported P values are two-sided and P < 0.05 was considered significant.
Results
All 4633 hip-fracture patients admitted during the 5-year study period from 2001 were included, and there were no cases lost to follow-up. Overall, 818 cases (17.7%) were not operated, this proportion varied from 10.3% to 23.6% among the hospitals. Hip fracture operations' types were distributed as follows: closed reduction of fracture of femur with internal fixation, 1371 (35.9%); Knowles nailing—close reduction of fracture of femur neck, 135 (3.5%); open reduction of fracture of femur with internal fixation, 350 (9.2%); Richard's hip nailing, 1803 (47.3%) and arthroplasty, 156 (4.1%). There was a variation in mean age and comorbidity scores among the hospitals: age ranging from 80.8 to 83.7 years and Charlson index from 4.3 to 4.7 points (P < 0.001 for both).
Table 1 depicts background characteristics of the patients stratified by the decision to operate and operation delay time. Male patients were somewhat younger (82.6 ± 7.3 vs. 81.3 ± 7.6 years, P < 0.001) than the females, but had a higher burden of comorbidities as reflected by Charlson index (4.6 ± 1.5 vs. 4.4 ± 1.2, P = 0.001). The proportion of males not operated was higher than that of female patients, 21.8%, 16.1%, respectively, P < 0.001. Non-operated patients were at the same age as those of operated patients (82.0 ± 7.5 vs. 82.3 ± 7.4 years, P = 0.26) and had higher comorbidity score (4.7 ± 1.3 vs. 4.4 ± 1.3, P < 0.001). The proportion of patients without additional registered diagnosis (comorbidity) was 22.2% and differed significantly among the hospitals (range 14.4% to 29.2%, P < 0.001).
Characteristics of the patients' population stratified by days elapsed from the admission to the operation
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Age (years) | 82.3 ± 7.4 | 82.0 ± 7.5 | 82.6 ± 7.5 | 81.6 ± 7.3 | 82.1 ± 7.0 | 0.0061 |
| Male gender (%) | 1264 (27.3) | 275 (33.6) | 613 (24.9) | 215 (28.8) | 61 (26.7) | <0.001 |
| Charlson index (median and IQ range) | 4.5 ± 1.3 | 4.7 ± 1.5 | 4.4 ± 1.2 | 4.4 ± 1.3 | 4.6 ± 1.5 | <0.0011 |
| Dementia (%) | 445 (9.6) | 97 (11.9) | 170 (6.9) | 92 (12.3) | 86 (14.2) | <0.0011 |
| Chronic ischemic heart disease (%) | 1096 (23.7) | 244 (29.8) | 518 (21.0) | 164 (22.0) | 170 (28.1) | <0.0011 |
| Diabetes (%) | 972 (21.0) | 184 (22.5) | 502 (20.4) | 158 (21.2) | 128 (21.2) | 0.63 |
| Hypertension (%) | 2151 (46.4) | 364 (44.5) | 1172 (47.5) | 329 (44.1) | 286 (47.4) | 0.23 |
| Atrial fibrillation (%) | 509 (11.0) | 121 (14.8) | 167 (6.8) | 111 (14.9) | 110 (18.2) | <0.0011 |
| Chronic obstructive pulmonary disease (%) | 262 (5.7) | 77 (9.4) | 115 (4.7) | 37 (5.0) | 33 (5.5) | <0.0011 |
| Hypothyroidism (%) | 282 (6.1) | 52 (6.4) | 137 (5.6) | 45 (6.0) | 48 (7.9) | 0.17 |
| Parkinson disease (%) | 235 (5.1) | 41 (5.0) | 107 (4.3) | 35 (4.7) | 52 (8.6) | <0.0011 |
| Solid organ or blood malignancy (%)2 | 130 (2.8) | 34 (4.2) | 59 (2.4) | 25 (3.4) | 12 (2.0) | 0.03 |
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Age (years) | 82.3 ± 7.4 | 82.0 ± 7.5 | 82.6 ± 7.5 | 81.6 ± 7.3 | 82.1 ± 7.0 | 0.0061 |
| Male gender (%) | 1264 (27.3) | 275 (33.6) | 613 (24.9) | 215 (28.8) | 61 (26.7) | <0.001 |
| Charlson index (median and IQ range) | 4.5 ± 1.3 | 4.7 ± 1.5 | 4.4 ± 1.2 | 4.4 ± 1.3 | 4.6 ± 1.5 | <0.0011 |
| Dementia (%) | 445 (9.6) | 97 (11.9) | 170 (6.9) | 92 (12.3) | 86 (14.2) | <0.0011 |
| Chronic ischemic heart disease (%) | 1096 (23.7) | 244 (29.8) | 518 (21.0) | 164 (22.0) | 170 (28.1) | <0.0011 |
| Diabetes (%) | 972 (21.0) | 184 (22.5) | 502 (20.4) | 158 (21.2) | 128 (21.2) | 0.63 |
| Hypertension (%) | 2151 (46.4) | 364 (44.5) | 1172 (47.5) | 329 (44.1) | 286 (47.4) | 0.23 |
| Atrial fibrillation (%) | 509 (11.0) | 121 (14.8) | 167 (6.8) | 111 (14.9) | 110 (18.2) | <0.0011 |
| Chronic obstructive pulmonary disease (%) | 262 (5.7) | 77 (9.4) | 115 (4.7) | 37 (5.0) | 33 (5.5) | <0.0011 |
| Hypothyroidism (%) | 282 (6.1) | 52 (6.4) | 137 (5.6) | 45 (6.0) | 48 (7.9) | 0.17 |
| Parkinson disease (%) | 235 (5.1) | 41 (5.0) | 107 (4.3) | 35 (4.7) | 52 (8.6) | <0.0011 |
| Solid organ or blood malignancy (%)2 | 130 (2.8) | 34 (4.2) | 59 (2.4) | 25 (3.4) | 12 (2.0) | 0.03 |
1P < 0.05 for comparison with non-operated patients excluded.
2Non-metastsatic prostate cancer excluded.
Characteristics of the patients' population stratified by days elapsed from the admission to the operation
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Age (years) | 82.3 ± 7.4 | 82.0 ± 7.5 | 82.6 ± 7.5 | 81.6 ± 7.3 | 82.1 ± 7.0 | 0.0061 |
| Male gender (%) | 1264 (27.3) | 275 (33.6) | 613 (24.9) | 215 (28.8) | 61 (26.7) | <0.001 |
| Charlson index (median and IQ range) | 4.5 ± 1.3 | 4.7 ± 1.5 | 4.4 ± 1.2 | 4.4 ± 1.3 | 4.6 ± 1.5 | <0.0011 |
| Dementia (%) | 445 (9.6) | 97 (11.9) | 170 (6.9) | 92 (12.3) | 86 (14.2) | <0.0011 |
| Chronic ischemic heart disease (%) | 1096 (23.7) | 244 (29.8) | 518 (21.0) | 164 (22.0) | 170 (28.1) | <0.0011 |
| Diabetes (%) | 972 (21.0) | 184 (22.5) | 502 (20.4) | 158 (21.2) | 128 (21.2) | 0.63 |
| Hypertension (%) | 2151 (46.4) | 364 (44.5) | 1172 (47.5) | 329 (44.1) | 286 (47.4) | 0.23 |
| Atrial fibrillation (%) | 509 (11.0) | 121 (14.8) | 167 (6.8) | 111 (14.9) | 110 (18.2) | <0.0011 |
| Chronic obstructive pulmonary disease (%) | 262 (5.7) | 77 (9.4) | 115 (4.7) | 37 (5.0) | 33 (5.5) | <0.0011 |
| Hypothyroidism (%) | 282 (6.1) | 52 (6.4) | 137 (5.6) | 45 (6.0) | 48 (7.9) | 0.17 |
| Parkinson disease (%) | 235 (5.1) | 41 (5.0) | 107 (4.3) | 35 (4.7) | 52 (8.6) | <0.0011 |
| Solid organ or blood malignancy (%)2 | 130 (2.8) | 34 (4.2) | 59 (2.4) | 25 (3.4) | 12 (2.0) | 0.03 |
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Age (years) | 82.3 ± 7.4 | 82.0 ± 7.5 | 82.6 ± 7.5 | 81.6 ± 7.3 | 82.1 ± 7.0 | 0.0061 |
| Male gender (%) | 1264 (27.3) | 275 (33.6) | 613 (24.9) | 215 (28.8) | 61 (26.7) | <0.001 |
| Charlson index (median and IQ range) | 4.5 ± 1.3 | 4.7 ± 1.5 | 4.4 ± 1.2 | 4.4 ± 1.3 | 4.6 ± 1.5 | <0.0011 |
| Dementia (%) | 445 (9.6) | 97 (11.9) | 170 (6.9) | 92 (12.3) | 86 (14.2) | <0.0011 |
| Chronic ischemic heart disease (%) | 1096 (23.7) | 244 (29.8) | 518 (21.0) | 164 (22.0) | 170 (28.1) | <0.0011 |
| Diabetes (%) | 972 (21.0) | 184 (22.5) | 502 (20.4) | 158 (21.2) | 128 (21.2) | 0.63 |
| Hypertension (%) | 2151 (46.4) | 364 (44.5) | 1172 (47.5) | 329 (44.1) | 286 (47.4) | 0.23 |
| Atrial fibrillation (%) | 509 (11.0) | 121 (14.8) | 167 (6.8) | 111 (14.9) | 110 (18.2) | <0.0011 |
| Chronic obstructive pulmonary disease (%) | 262 (5.7) | 77 (9.4) | 115 (4.7) | 37 (5.0) | 33 (5.5) | <0.0011 |
| Hypothyroidism (%) | 282 (6.1) | 52 (6.4) | 137 (5.6) | 45 (6.0) | 48 (7.9) | 0.17 |
| Parkinson disease (%) | 235 (5.1) | 41 (5.0) | 107 (4.3) | 35 (4.7) | 52 (8.6) | <0.0011 |
| Solid organ or blood malignancy (%)2 | 130 (2.8) | 34 (4.2) | 59 (2.4) | 25 (3.4) | 12 (2.0) | 0.03 |
1P < 0.05 for comparison with non-operated patients excluded.
2Non-metastsatic prostate cancer excluded.
Of the 3815 patients who underwent surgery, 1350 (35.4%) waited for >2 days to be operated. The median pre-operative stay for the entire cohort was 1 day with an inter quartile (IQ) range of 0–3 days. There was a substantial variation in pre-operative delay among the hospitals, with median time ranging from 0 (Hospitals 1, 2, 5) to 4 days (Hospital 4), P < 0.001. Similarly, the inter-hospital variability in proportion of patients operated within 2 days was high, ranging from 20.3% to 78.6% (P < 0.001). There was no correlation between the number hip operations and the proportion of patients operated within 2 days (Spearman's ρ = −0.29, P = 0.54). Surgery delay time was not affected by the admission day of the week—patients hospitalized on Thursday–Friday–Saturday (weekend) were operated within the same time-frame as those admitted on the weekdays (P = 0.19).
Table 2 reveals hospitalization characteristics, short- and long-term outcomes of the patients' population stratified by the decision to operate and operation delay time. Patients who had surgery within 2 days had lower mortality (in-hospital, 1-month and 1-year) compared to those who waited for surgery >4 days. Total length of stay varied considerably among the hospitals, ranging from median of 6.0 (Hospital 3) to 21.0 days (Hospital 4), P < 0.001. From 4424 patients survived to the hospital discharge, 288 patients (6.5%) were discharged to rehabilitation facilities. The median length of stay for this group of patients (10.0 days, IQ range 7.0 to 14 days) did not differ from the group of patients discharge to home (9.0 days, IQ range 6.0–15.0 days), P = 0.17. Multivariate linear regression analysis demonstrated that after adjustment for background comorbidities (Charlson score) and age, every additional day of surgery delay resulted in longer post-operation hospital stay (P < 0.001).
Hospitalization characteristics and short- and long-term outcomes of the patients' population stratified by the decision to operate and pre-operative stay
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Total length of stay, days (median and IQ range) | 9.0 (6.0–15.0) | 8.0 (3.0–16.0) | 8.0 (6.0–12.0) | 10.0 (8.0–19.0) | 16.0 (11.0–27.0) | <0.0011 |
| Length of stay after operation, days (median and IQ range) | 7.0 (5.0–12.0) | 7.0 (5.0–11.0) | 7.0 (5.0–16.0) | 9.0 (5.0–20.0) | <0.001 | |
| Readmission within one month (%)2 | 525 (11.3) | 114 (13.9) | 240 (9.7) | 91 (12.2) | 80 (13.2) | <0.0021 |
| In-hospital mortality (%) | 209 (4.5) | 89 (10.9) | 71 (2.9) | 21 (2.8) | 28 (4.6) | <0.001 |
| 1-month mortality (%) | 278 (6.0) | 109 (13.3) | 99 (4.0) | 33 (4.4) | 37 (6.1) | <0.001 |
| 1-Year mortality (%) | 1038 (22.4) | 296 (36.2) | 429 (17.4) | 155 (20.8) | 158 (26.2) | <0.0011 |
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Total length of stay, days (median and IQ range) | 9.0 (6.0–15.0) | 8.0 (3.0–16.0) | 8.0 (6.0–12.0) | 10.0 (8.0–19.0) | 16.0 (11.0–27.0) | <0.0011 |
| Length of stay after operation, days (median and IQ range) | 7.0 (5.0–12.0) | 7.0 (5.0–11.0) | 7.0 (5.0–16.0) | 9.0 (5.0–20.0) | <0.001 | |
| Readmission within one month (%)2 | 525 (11.3) | 114 (13.9) | 240 (9.7) | 91 (12.2) | 80 (13.2) | <0.0021 |
| In-hospital mortality (%) | 209 (4.5) | 89 (10.9) | 71 (2.9) | 21 (2.8) | 28 (4.6) | <0.001 |
| 1-month mortality (%) | 278 (6.0) | 109 (13.3) | 99 (4.0) | 33 (4.4) | 37 (6.1) | <0.001 |
| 1-Year mortality (%) | 1038 (22.4) | 296 (36.2) | 429 (17.4) | 155 (20.8) | 158 (26.2) | <0.0011 |
1P < 0.05 for comparison with non-operated patients excluded.
2Percentage from 4604 patients discharged after initial hospitalization.
Hospitalization characteristics and short- and long-term outcomes of the patients' population stratified by the decision to operate and pre-operative stay
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Total length of stay, days (median and IQ range) | 9.0 (6.0–15.0) | 8.0 (3.0–16.0) | 8.0 (6.0–12.0) | 10.0 (8.0–19.0) | 16.0 (11.0–27.0) | <0.0011 |
| Length of stay after operation, days (median and IQ range) | 7.0 (5.0–12.0) | 7.0 (5.0–11.0) | 7.0 (5.0–16.0) | 9.0 (5.0–20.0) | <0.001 | |
| Readmission within one month (%)2 | 525 (11.3) | 114 (13.9) | 240 (9.7) | 91 (12.2) | 80 (13.2) | <0.0021 |
| In-hospital mortality (%) | 209 (4.5) | 89 (10.9) | 71 (2.9) | 21 (2.8) | 28 (4.6) | <0.001 |
| 1-month mortality (%) | 278 (6.0) | 109 (13.3) | 99 (4.0) | 33 (4.4) | 37 (6.1) | <0.001 |
| 1-Year mortality (%) | 1038 (22.4) | 296 (36.2) | 429 (17.4) | 155 (20.8) | 158 (26.2) | <0.0011 |
| All patients (N = 4633) | Days to operation | P-value | ||||
|---|---|---|---|---|---|---|
| No operation (N = 818) | <2 days (N = 2465) | 2–4 days (N = 746) | >4 days (N = 604) | |||
| Total length of stay, days (median and IQ range) | 9.0 (6.0–15.0) | 8.0 (3.0–16.0) | 8.0 (6.0–12.0) | 10.0 (8.0–19.0) | 16.0 (11.0–27.0) | <0.0011 |
| Length of stay after operation, days (median and IQ range) | 7.0 (5.0–12.0) | 7.0 (5.0–11.0) | 7.0 (5.0–16.0) | 9.0 (5.0–20.0) | <0.001 | |
| Readmission within one month (%)2 | 525 (11.3) | 114 (13.9) | 240 (9.7) | 91 (12.2) | 80 (13.2) | <0.0021 |
| In-hospital mortality (%) | 209 (4.5) | 89 (10.9) | 71 (2.9) | 21 (2.8) | 28 (4.6) | <0.001 |
| 1-month mortality (%) | 278 (6.0) | 109 (13.3) | 99 (4.0) | 33 (4.4) | 37 (6.1) | <0.001 |
| 1-Year mortality (%) | 1038 (22.4) | 296 (36.2) | 429 (17.4) | 155 (20.8) | 158 (26.2) | <0.0011 |
1P < 0.05 for comparison with non-operated patients excluded.
2Percentage from 4604 patients discharged after initial hospitalization.
Within 30 days after initial hospitalization, 525 (11.9%) of the discharged patients were readmitted. Readmission was highest for patients not operated on (13.9%) and was lowest for patients operated within 2 days (9.7%). The most common primary diagnoses at readmission were as follows: non-infectious complication of the operation site, 104 (2.3%) patients, surgical wound infection, 29 (0.6%) patients and other infections such as pneumonia, urinary tract infection etc., 142 (3.1%) patients, acute-coronary syndrome and pulmonary oedema, 25 (0.5%) patients, veno-thromboembolism, 16 (0.3%) patients and bleeding (other than from operation site), 23 (0.5%) patients. Out of 525 readmitted patients, only 91 (17.3%) were hospitalized in orthopedic departments, while the majority was admitted to internal medicine wards.
The relative risks of in-hospital, 1-month and 1-year mortality of non-operated compared to operated patients were 3.5 (95% CI, 2.7–4.5), 3.0 (95% CI, 2.4–3.8) and 1.9 (95% CI, 1.7–2.1), respectively. Figure 1 depicts the cumulative survival of patients with and without surgery for hip fracture (log-rank test, P < 0.001). Analysing Kaplan–Meier curves only in operated patients yielded similar results—shorter operation delay time was associated with better 1-year survival (log-rank test, P < 0.001). A Cox proportional regression model of 1-year mortality (Table 3) adjusted for comorbidity, age and gender shows that the length of operation delay has a gradual effect on increasing mortality.
Kaplan–Meier survival functions by the pre-operative stay.
Cox proportional hazard regression model for 1-year mortality prediction in a cohort of 4633 patients hospitalized after hip fracture
| Hazard ratio | 95.0% CI | P-value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Days of hospitalization before surgery1 | ||||
| <2 | 1 | |||
| 2–4 | 1.20 | 1.00 | 1.44 | 0.05 |
| >4 | 1.50 | 1.20 | 1.80 | <0.001 |
| Not operated | 2.23 | 1.92 | 2.60 | <0.001 |
| Age, per category2 | 1.16 | 1.08 | 1.25 | <0.001 |
| Gender, female vs. male | 0.72 | 0.63 | 0.82 | <0.001 |
| Charlson index, per point | 1.32 | 1.27 | 1.37 | <0.001 |
| Arterial hypertension | 0.79 | 0.69 | 0.89 | <0.001 |
| Hazard ratio | 95.0% CI | P-value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Days of hospitalization before surgery1 | ||||
| <2 | 1 | |||
| 2–4 | 1.20 | 1.00 | 1.44 | 0.05 |
| >4 | 1.50 | 1.20 | 1.80 | <0.001 |
| Not operated | 2.23 | 1.92 | 2.60 | <0.001 |
| Age, per category2 | 1.16 | 1.08 | 1.25 | <0.001 |
| Gender, female vs. male | 0.72 | 0.63 | 0.82 | <0.001 |
| Charlson index, per point | 1.32 | 1.27 | 1.37 | <0.001 |
| Arterial hypertension | 0.79 | 0.69 | 0.89 | <0.001 |
1Patients' group operated within <2 days served as a reference group.
2Age grouped into four categories: <70, 70–80, 80–90 and >90 years.
Cox proportional hazard regression model for 1-year mortality prediction in a cohort of 4633 patients hospitalized after hip fracture
| Hazard ratio | 95.0% CI | P-value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Days of hospitalization before surgery1 | ||||
| <2 | 1 | |||
| 2–4 | 1.20 | 1.00 | 1.44 | 0.05 |
| >4 | 1.50 | 1.20 | 1.80 | <0.001 |
| Not operated | 2.23 | 1.92 | 2.60 | <0.001 |
| Age, per category2 | 1.16 | 1.08 | 1.25 | <0.001 |
| Gender, female vs. male | 0.72 | 0.63 | 0.82 | <0.001 |
| Charlson index, per point | 1.32 | 1.27 | 1.37 | <0.001 |
| Arterial hypertension | 0.79 | 0.69 | 0.89 | <0.001 |
| Hazard ratio | 95.0% CI | P-value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Days of hospitalization before surgery1 | ||||
| <2 | 1 | |||
| 2–4 | 1.20 | 1.00 | 1.44 | 0.05 |
| >4 | 1.50 | 1.20 | 1.80 | <0.001 |
| Not operated | 2.23 | 1.92 | 2.60 | <0.001 |
| Age, per category2 | 1.16 | 1.08 | 1.25 | <0.001 |
| Gender, female vs. male | 0.72 | 0.63 | 0.82 | <0.001 |
| Charlson index, per point | 1.32 | 1.27 | 1.37 | <0.001 |
| Arterial hypertension | 0.79 | 0.69 | 0.89 | <0.001 |
1Patients' group operated within <2 days served as a reference group.
2Age grouped into four categories: <70, 70–80, 80–90 and >90 years.
The crude 1-year mortality rate for entire population was 22.4% (95% CI, 21.2–23.7), ranging from 21.0% to 25.1% in individual hospitals (P = 0.78). Cox regression model for evaluating hospital-adjusted mortality variation was built with Hospital 0 (lowest mortality) serving as a reference group. According to this model, Hospitals 1, 2 and 4 had excess 1-year mortality risk, 1.35 (95% CI, 1.04–1.76), 1.36 (95% CI, 1.07–1.72) and 1.45 (95% CI, 1.11–1.88), respectively. Pre-operative delay retained its significance: patients operated between 2 and 4 days had 1-year mortality hazard ratio of 1.24 (95% CI, 1.03–1.50), patients operated after 4 days had 1.60 (95% CI, 1.32–1.96) and non-operated patients had 2.32 (95% CI, 1.98–2.71) compared to the patients operated within 2 days.
In order to assess the potential effect of under-reporting of the comorbidity, we performed survival analysis in subgroup of patients with at least one additional diagnosis. This analysis corroborated the 1-year mortality surplus in patients operated between days 2 and 4 of the hospitalization (hazard ratio 1.24, 95% CI, 1.01–1.52), after 4 days (hazard ratio 1.56, 95% CI, 1.27–1.90) or those treated conservatively (hazard ratio 2.27, 95% CI, 2.27–2.68) compared to the group that was operated within 2 days.
Discussion
The current data shows an average performance of 53.2% of patients operated within 2 days, within the range of performance reported by western countries of 33% to 93% [11]. Our data confirm the previous reports on the association between delayed surgery and increased mortality in elderly patients admitted for hip fracture repair. Delay in hip fracture surgery is significantly associated with increased risk of mortality, even after controlling for patients characteristics. Similar to others, we found that increased risk of mortality extends beyond the hospital phase [8], and persists at least up to 1 year after admission. It is readily understandable that delays in surgery after hip fracture in an elderly population can lead to increased short-term mortality, perhaps due to the increased risk of prolonged immobilization, increased hospital length of stay and increased risk of infection. It is somewhat surprising that this increased risk persisted for 1 year suggesting that other less identifiable factors are also playing a role.
Advances in surgical and anaesthetic techniques make early surgery of high-risk elderly patients a promising reality. Yet, in the current study, 17.7% of the patients were not operated upon, more than in a recent report from the UK—no recorded surgery in 7.1% of the patient population [8]. It seems that in this population of patients in their eighties, some medical centres practiced a more conservative approach. If operative treatment is refused or the risks of surgery are considered to be too high, the main emphasis of treatment is on pain relief. Severe impairments in functional status such as previous immobility or impaired mental status could have brought to a decision not to operate upon. However, surgical delay cannot be attributed entirely to the patients' condition, as we have found substantial variation in pre-operative time among the hospitals. Therefore, the hospitals' variation in the operation delay time can be addressed as a pseudo-randomization of the study population. Thus, it can be assumed that timing of the operation is at least partly related to the worse outcome.
Our study confirmed that surgical delay was associated with longer post-surgical hospital stay, independent of the presence of comorbidity or increasing age [14]. Similar to 1-year mortality, we found substantial inter-hospital variations in operation delay time.
The current analysis neither proves a cause-and-effect role of timely surgery on clinical outcomes, nor indicates which factors withhold better hospital performance, but clearly points to major variations in process and outcome among the hospitals. Reducing variation is possible by embarking upon quality improvement initiatives and benchmarking. If improving the performance by shortening the time to surgery and reducing the variation will lead to a reduction in mortality, then the present observed association between surgical delays and mortality could indicate causality. Furthermore, reduction in delays can potentially reduce the length of hospital stay and cut costs.
The proportion of the patients with hip surgery delay for >2 days in the present report and the wide variation in operation delay time among hospitals are a troubling finding. Need for medical stabilization and operational logistics are common reasons for withholding operations. While medical stabilization is understandably a necessity, it should be done in a mode that optimizes time to surgery. Operational delays, on the other hand, should be addressed differently, using management tools such as fast tracks, and incentives to teams to meet targets.
Our study has several potential limitations. Time to surgery was computed based on the dates of admission and surgery, and was not refined to actual hour of surgery, which might introduce a bias into the estimation of the operative delay effect. The quality of administrative hospital discharge data is always of concern, and although hip fracture diagnosis and procedures tend to be relatively straightforward abstractions, comorbid conditions were recorded in secondary discharge diagnoses that may be incomplete. We lacked data on socio-economical status and of functional status prior to admission, two factors that may have affected patient selection for surgery, time to surgery, and the outcome of these elderly patients. Given the retrospective design of the present study, one can assume that early surgery may be a surrogate of closer medical attention and reflect a ‘better’ overall health status of the patient. To adjust for this potential confounder, we introduced Charlson comorbidity index, that is often used for case-mix adjustment in studies of hip fracture management [15–17]. However, potential residual confounding cannot be excluded. Furthermore, in analysing database-derived information on coded diagnosis, we must be aware of the possible errors from incorrect or lack of coding.
In summary, we have shown that delaying surgery after hip fracture is associated with worse outcomes. Reducing variations among hospitals and improving performance according to guidelines, make surgery for hip replacement a prime candidate for quality improvement activities in medical organizations. Our data supports the notion that deviating from surgical guidelines in hip fracture is costly, both in terms of human life and of excess hospital stay.

{kind=link}
{kind=link}