
Abstract
Purpose
This article is a review of the efficacy and safety of the Laryngeal Mask Airway (LMA) Supreme™ as a stand-alone supraglottic airway during general anesthesia and as a conduit for tracheal intubation. Relevant articles were obtained using MEDLINE (1948-July 2011) and EMBASE (1980-July 2011). Only original studies with adult human patients and published in English were selected.
Principal findings
The LMA Supreme was found to be comparable with the LMA Proseal™ with regard to success rate, insertion time, and complications. However, in three studies, oropharyngeal leak pressure was higher with the LMA Proseal than with the LMA Supreme. The LMA Supreme was superior to the LMA Classic™ with regard to insertion time and oropharyngeal seal pressure. The LMA Supreme was also used successfully in two difficult airway cases, and it has been used as a conduit for tracheal intubation by utilizing an intubation introducer (gum elastic bougie) and subsequently railroading an endotracheal tube over the bougie into the trachea. Techniques for achieving tracheal intubation include the use of the Aintree Intubation Catheter®, a guidewire-exchange catheter, a gum elastic bougie, and a small (<6.0 mm internal diameter) endotracheal tube.
Conclusion
The LMA Supreme has been shown to be a safe and efficacious device as a stand-alone supraglottic airway and may also be used as a conduit for tracheal intubation. Further trials are needed to determine the efficacy of the LMA Supreme compared with other supraglottic airways in both elective and emergent airway management situations.
Résumé
Objectif
Cet article est une analyse de l’efficacité et de l’innocuité du masque laryngé (LMA) Supreme™ utilisé seul comme dispositif supraglottique au cours d’une anesthésie générale et comme conduit pour l’intubation trachéale. Les articles pertinents ont été identifiés en recherchant dans les bases de données MEDLINE (1948 à juillet 2011) et EMBASE (1980 à juillet 2011). Seules ont été sélectionnées les études originales portant sur des patients humains adultes et publiées en anglais.
Constatations principales
On a trouvé que le LMA Supreme est comparable au LMA Proseal™ en termes de taux de succès, de temps d’insertion et de complications. Cependant, dans trois études, la pression de fuite oropharyngée était plus élevée avec le LMA Proseal qu’avec le LMA Supreme. Le LMA Supreme était supérieur au LMA Classic™ pour ce qui concerne le temps d’insertion et la pression d’étanchéité oropharyngée. Le LMA Supreme a également été utilisé avec succès dans deux cas d’intubation difficile et a servi de guide pour une intubation trachéale en utilisant un mandrin d’intubation souple (gum elastic bougie) puis en faisant glisser la sonde endotrachéale le long du mandrin dans la trachée. Les techniques permettant d’obtenir une intubation trachéale incluent l’utilisation d’un cathéter d’intubation d’Aintree®, un échangeur de tube, un mandrin souple et une petite sonde endotrachéale (<6,0 mm de diamètre intérieur).
Conclusion
Le LMA Supreme s’est avéré sûr et efficace comme dispositif supraglottique autonome et peut aussi être utilisé comme conduit en vue d’une intubation trachéale. D’autres études sont nécessaires pour établir l’efficacité du LMA Supreme par rapport aux autres dispositifs supraglottiques pour la prises en charge des voies aériennes aussi bien dans les situations programmées que dans les situations d’urgence.
Similar content being viewed by others


Following the introduction of the Laryngeal Mask Airway (LMA) Classic™ (LMA™ North America, Inc., San Diego, CA, USA) in the 1980 s, the use of laryngeal mask airway devices in elective and emergent airway management has become widespread in clinical practice. The role of the LMA Classic during general anesthesia, both as a ventilation device and as a conduit for intubation, has been amply described in literature.1-3 Since then, newer supraglottic airway models have been introduced. The LMA Proseal™, (LMA™ North America, Inc., San Diego, CA, USA) developed in 2000, consists of a double lumen which separates the respiratory and alimentary tracts, improving protection from aspiration.4-6 Compared with the LMA Classic, the modified inflatable cuff of the LMA Proseal has higher oropharyngeal leak pressure around the laryngeal outlet.7 It has also been used as an acceptable alternative to the endotracheal tube in situations with potential gastric aspiration, such as in Cesarean delivery or laparoscopic surgery.8,9 The LMA Proseal is thus considered the standard “state of the art” supraglottic airway, and it should be used as the standard of comparison for newly developed supraglottic airways.
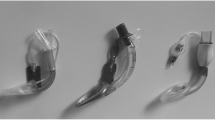
The LMA Supreme™, (LMA™ North America, Inc., San Diego, CA, USA) developed in 2007, is a modified single-use version of the LMA Proseal. Its preformed curved shaft consists of a double lumen, i.e., a central lumen for access to the digestive tract encased within a flattened oval-shaped airway lumen for access to the respiratory tract.10-13 Other features of the LMA Supreme include a built-in bite block to prevent airway obstruction due to patient bite and moulded fins at the laryngeal outlet to prevent epiglottic obstruction (Fig. 1).

Frontal (left) and side (right) views of the LMA Supreme. ET = epiglottic fins; FT = fixation tab
The LMA Supreme is inserted with the cuff fully deflated, and it is recommended that lubrication be applied to the posterior surface of the airway and cuff to facilitate passage into the airway. With the patient positioned in a semi-sniffing position, the device is advanced with the distal tip flat along the hard palate. The device is then rotated inwards using a single hand, similar to the LMA Fastrach™, until resistance is felt. If correctly positioned, the tip of the cuff should rest at the esophageal inlet. The cuff is then inflated to the standard intracuff pressure of 60 mmHg.11,14 The LMA Supreme is usually fixated by taping across the fixation tab, with the tab situated 1-2.5 cm from the patient’s upper lip. If the fixation tab is < 1 cm or > 2.5 cm from the upper lip, this suggests that the size of airway device is either too small or too big, respectively. Since its release, the LMA Supreme has been used both as a supraglottic airway for ventilation during general anesthesia and as a conduit for tracheal intubation. This article is a review of the efficacy and safety of the LMA Supreme as a stand-alone device and as a conduit for tracheal intubation.
We used the MEDLINE (1948-July 2011) and EMBASE (1980-July 2011) databases to find potential articles, and the keywords “LMA Supreme” and “sLMA” were used in the search. Nineteen articles were found, 12 of which reported randomized controlled trials (RCTs) comparing the LMA Supreme with other airway devices; seven articles were prospective single-device studies and four were case reports. We assessed a number of outcomes of interest, including insertion success, insertion time, oropharyngeal leak pressure, and complications. The characteristics and outcomes of the studies are listed in Tables 1 and 2, respectively.
Use of LMA Supreme in normal airway/elective surgery
Comparison of the LMA Supreme and LMA Proseal
We located 12 published RCTs examining use of the LMA Supreme as a stand-alone supraglottic airway (Table 1). Six of the studies compared the LMA Supreme with the LMA Proseal.10,13-17 The remaining studies compared the LMA Supreme with the LMA Classic,23 i-gel,18-20 facemask,21 or endotracheal tube.22
In the six RCTs comparing the LMA Supreme with the LMA Proseal, 418 patients were identified and 295 (70%) of those were female. Three of the six trials were parallel randomized controlled trials, while the other three were crossover RCTs. All patients were undergoing elective surgery, and those with an anticipated difficult airway were excluded from the study. A summary of the study outcomes are listed in Table 2. Success rates were similar between the two airway devices in all studies. Overall insertion success rates were 100% for both the LMA Supreme and LMA Proseal. First attempt success rates were similar and ranged from 90-98% for the LMA Supreme and 83-97% for the LMA Proseal.
Insertion end times were defined differently in each study. End points included placement of the LMA,13 obtaining effective airway/ventilation,14,17 connection to the anesthesia circuit,10 and obtaining a satisfactory capnography tracing.15 Despite subtle differences in end points, insertion times were similar between the LMA Supreme and LMA Proseal in all studies.
Oropharyngeal leak pressure associated with the LMA Supreme and LMA Proseal was assessed. In three studies, oropharyngeal leak pressure with the LMA Proseal was significantly higher than that with the LMA Supreme,13,15,17 but it did not differ significantly in the other three studies.10,14,16 In a study by Hosten et al., leak pressure was comparable between groups at one minute and at 60 min after insertion of the airway device; however, the pressure within both groups at 60 min was significantly lower compared with the pressure at one minute.14
Five of the studies recorded complications, including blood staining on the airway device and sore throat (Table 2).13-17 Complications were infrequent and did not differ appreciably between devices. Overall, the incidence of blood staining was 18/207 (9%) with the LMA Proseal compared with 13/208 (6%) with the LMA Supreme. Lee et al. also reported just three occurrences of sore throat for both devices and one case of hoarseness with the LMA Proseal.17
Comparison of LMA Supreme with other airway devices
In six randomized controlled studies, the LMA Supreme was compared with other airway devices, including the face mask, endotracheal tube, LMA Classic, and i-gel.
Comparison of the LMA Supreme and i-gel
Three RCTs compared the LMA Supreme with i-gel.18-20 Two hundred fifty patients were identified and 191 (76%) of those were female. All patients were undergoing elective surgery. Two studies compared the devices in situations of a predicted normal airway,19,20 but in the third study, the devices were assessed in the context of a difficult airway through simulation using an extrication collar.18 The first attempt and overall success rates were high but not significantly different, ranging from 93-98% and 85-96% on first attempt and 94-100% and 93-100% overall with the LMA Supreme and i-gel, respectively.
Airway insertion time was defined differently in each study. Ranges included time from removal of the facemask to successful ventilation,18 from picking up the device to obtaining the first end-tidal CO2 tracing,19 and time from insertion of the device to first end-tidal CO2 tracing.20 In one study, insertion times were faster with the LMA Supreme than with the i-gel [34 (12) sec vs 42 (23) sec; P = 0.024],18 but they were not significant in the other two studies.19,20
In one study, the oropharyngeal leak pressure was found to be higher with the LMA Supreme than with the i-gel,19 but it was not significant in the other studies.18,20 Complications were infrequent with both devices. Due to the crossover nature of Theiler et al.’s study, postoperative discomfort could not be determined.18
Comparison of the LMA Supreme with the facemask
The LMA Supreme was compared with the facemask in 31 morbidly obese patients with difficult facemask ventilation predictors.21 After brief training, ten medical students, novel to airway management, performed the facemask and LMA Supreme airway management techniques. Ventilation using the facemask was successful in 27/31 (87%) cases while ventilation using the LMA Supreme was successful in 31/31 (100%) cases. The insertion time, from picking up each device to the first CO2 tracing, was significantly higher with the ventilation facemask than with the LMA Supreme [34 (14) sec vs 21 (9) sec, respectively; P < 0.05].
Comparison of the LMA Supreme and endotracheal tube
The LMA Supreme was also compared with the endotracheal tube.22 One hundred thirty-eight female patients undergoing elective surgery were randomized into either device arm, and there were no insertion failures with either device. Time to successful airway placement, from injection of atracurium to definitive ventilation, was 3.8 (0.7) min for the endotracheal tube and 2.2 (0.6) min for the LMA Supreme (non-significant). Oropharyngeal leak pressure was > 30 cm H2O in 95% of cases with the LMA Supreme and in 100% of cases with the endotracheal tube. Postoperative discomfort, such as hoarseness of voice, dysphagia, and sore throat were significantly higher in the endotracheal tube group (P < 0.05).
Comparison of the LMA Supreme and LMA Classic
The LMA Supreme was compared with the LMA Classic in 70 patients undergoing surgery.23 Insertion success on first attempt was 27/35 (77%) using the LMA Classic and 31/35 (88%) using the LMA Supreme, and overall insertion success was 31/35 (89%) and 34/35 (97%), respectively (non-significant). Insertion time was faster with the LMA Supreme than with the LMA Classic [8 (1.7) sec vs 11.2 (2.5) sec, respectively; P < 0.001]. Oropharyngeal leak pressure was also higher with the LMA Supreme than with the LMA Classic [34.6 (3.1) cm H2O vs 26.1 (2.1) cm H2O, respectively; P < 0.001]. An adverse effects assessment for nausea and vomiting, agitation, and sore throat was conducted one hour post-operation, and no statistical significance was found between the two groups.
Thus, the LMA Supreme was shown to be comparable with the LMA Proseal with regard to airway success rate, device insertion time, and a favourable complication profile. However, in three of the six studies, oropharyngeal leak pressure was significantly higher in the LMA Proseal than in the LMA Supreme. When compared with the i-gel, the LMA Supreme was comparable with respect to success rates and complications, but some studies indicated a shorter insertion time and higher oropharyngeal leak pressure compared with the LMA Supreme. There are insufficient data to formulate conclusions when comparing the LMA Supreme with the facemask, endotracheal tube, and LMA Classic.
LMA Supreme: prospective single-device studies
The LMA Supreme has been investigated in seven prospective controlled single-device studies involving 507 patients undergoing general anesthesia 11, 12, 24–28 (Table 2). Together, these studies showed overall insertion success in 616/617 (99.8%) patients using the LMA Supreme. Insertion success ranged from 86-100% of patients on first attempt. Insertion times were reported in six studies but were poorly defined in four studies.11,12,24,28 In studies where the end points of insertion times were defined, they were defined either as time to connection of breathing system25 or as time to first ventilation.27 The oropharyngeal leak pressure observed in four studies ranged from 23-39 cm H2O.12,24,25,27 There was a low incidence of complications, including sore throat, vomiting, pain on swallowing, and upper airway trauma. Blood staining was recorded in two studies and was infrequent, 10/140 patients (7%).25,28
Use of the LMA Supreme in difficult airway/emergent situations
Four case reports have shown successful insertion using the LMA Supreme in difficult airway situations. One case involved insertion of the LMA Supreme in a patient undergoing elective surgery,29 and another case involved a patient with ventricular fibrillation requiring chest compression.30 The remaining two cases documented successful insertions in patients whose lungs were difficult to ventilate due to partially obstructed airways.31,32 One LMA Supreme insertion was later replaced with a tracheostomy tube due to an anticipated difficult endotracheal intubation.31 The LMA Supreme was also inserted successfully in 57/60 (95%) cases of simulated difficult airway.18 In a simulated difficult airway, use of the LMA Supreme was associated with a faster insertion time compared with the i-gel. Due to a limited number of reports involving the LMA Supreme as a ventilator device in difficult airway situations, there is insufficient data to conclude about its efficacy in such cases; therefore, additional studies are needed.
Use of LMA Supreme as a conduit for tracheal intubation
In a cannot intubate, cannot ventilate or a failed intubation situation, a supraglottic airway, such as the LMA Classic or LMA Supreme, can be used as a temporary rescue airway and can also serve as a conduit for intubation.33,34 Due to the limited airway luminal diameter of the LMA Supreme, it is difficult to pass an endotracheal tube of adequate size directly through it. Thus, a variety of techniques, mainly via the use of introducers or catheters, have been developed to achieve tracheal intubation with the LMA Supreme. There are four reported techniques using an Aintree Intubation Catheter,35,36 a guidewire-catheter,36,37 a gum elastic bougie,38 or a small endotracheal tube.39
The first technique, which utilizes the Aintree Intubation Catheter, was described by Joffe et al. in a mannequin setting with 20 participants.36 The Aintree Intubation Catheter (4.7-mm internal diameter, 6.3-mm outer diameter) was mounted over a flexible bronchoscope (Fig. 2). Once mounted, the bronchoscope-Aintree assembly was then inserted through the LMA Supreme into the trachea where mean time to completion was 54 (21) sec. After the bronchoscope and LMA Supreme were withdrawn, an endotracheal tube was railroaded over the Aintree Intubation Catheter. There were two failures; in one case, the Aintree Intubation Catheter was dislodged during removal of the LMA Supreme, and in the other case, the bronchoscope-Aintree assembly failed to maneuver past the vocal cords.

(Top) Aintree Intubation Catheter is placed over a flexible bronchoscope. (Bottom) An Aintree Intubation Catheter/bronchoscope complex is inserted through a LMA Supreme
The second technique, utilizing a guidewire, was described in three patients in a mannequin setting.36,37 A guidewire was inserted through the lumen of the bronchoscope, and then both were inserted through the LMA Supreme into the trachea. After removal of the bronchoscope and LMA Supreme, the guidewire was exchanged for an Arndt Exchange Catheter. Subsequently, an endotracheal tube was railroaded over the Arndt Exchange Catheter. In the report by Joffe et al., 36 they compared tracheal intubation with the Aintree Intubation Catheter vs intubation with the Arndt Exchange Catheter Set. Twenty experienced anesthesiologists used an LMA Supreme to perform each method once on an AirSim airway mannequin. Intubation was 90% successful using an Aintree Intubation Catheter and 100% successful using the guidewire. However, faster intubation was achieved with the Aintree Intubation Catheter technique vs the guidewire [54 (21) sec vs 98 (23) sec, respectively; P < 0.0001].
In the third technique, which involved four patients with a normal airway who were undergoing elective surgery, Mathes et al. 38 described insertion of a gum elastic bougie in combination with a flexible bronchoscope through the respiratory lumen of the LMA Supreme. The bronchoscope and LMA Supreme were then removed, and an endotracheal tube was railroaded over the bougie into the trachea. Success was achieved in two of the four patients. In a variation of this technique, a nasogastric tube was used as an adjunct for tracheal intubation through the LMA Supreme in four patients with a normal airway who were undergoing elective surgery. The bronchoscope was first inserted into a nasogastric tube before passing through the LMA Supreme. The bronchoscope was then exchanged for a bougie, followed by removal of the LMA Supreme. An endotracheal tube was then railroaded over the nasogastric tube/bougie into the trachea. Success was achieved in all four cases.
Lastly, in the fourth technique described by Carron et al.,39 a small endotracheal tube was used as an intermediary for a larger tube in a patient with three failed attempts at laryngoscopic tracheal intubation. A size 4 LMA Supreme was first inserted for ventilation. A small endotracheal tube (6.0-mm internal diameter) was then mounted over a bronchoscope and inserted through the LMA Supreme into the trachea. The bronchoscope and LMA Supreme were withdrawn, and a 4.0-mm Cook Airway Exchange Catheter was inserted into the small endotracheal tube. Subsequently, the small endotracheal tube was removed and a 7.5-mm internal diameter endotracheal tube was railroaded into the trachea.
The above reports suggest that the LMA Supreme in combination with introducers/catheters can be a viable alternative to achieve tracheal intubation. However, there are limited data to support the efficacy of this device as a conduit for tracheal intubation in difficult intubation situations.
Limitations
There are a number of limitations which affect the interpretation of these data. It is difficult to generate solid conclusions with a limited number of RCTs with sufficient power to compare the LMA Supreme with other airway devices. Heterogeneity in the definition of outcomes, including airway device insertion time, makes it difficult to draw comparisons between studies. In addition, there are few studies documenting the use of the LMA Supreme in difficult airway situations or as a conduit for intubation. Thus, additional RCTs are needed.
Conclusions
The LMA Supreme is a single-use version of the reusable double-lumen LMA Proseal. With the built-in pre-shaped shaft, it can be inserted in the same fashion as the LMA Fastrach. The efficacy and safety of the LMA Supreme as a stand-alone supraglottic airway has been shown in a number of studies. Insertion success, insertion time, and incidence of complications were shown to be comparable with the LMA Proseal in patients with normal airways. In several studies, the LMA Proseal was shown to have higher oropharyngeal leak pressure than the LMA Supreme. Furthermore, the LMA Supreme has been used successfully in a limited number of difficult airway cases. The LMA Supreme can be used as a conduit for tracheal intubation through the use of introducers or catheters. Definitive outcome-based clinical trials that are conducted meticulously, powered appropriately, and reported transparently are required to compare the efficacy of the LMA Supreme with other supraglottic airway devices in both elective and emergency airway management settings.
References
Verghese C, Brimacombe JR. Survey of laryngeal mask airway usage in 11,910 patients: safety and efficacy for conventional and nonconventional usage. Anesth Analg 1996; 82: 129-33.
Brimacombe J. Analysis of 1500 laryngeal mask uses by one anaesthetist in adults undergoing routine anaesthesia. Anaesthesia 1996; 51: 76-80.
Campo SL, Denman WT. The laryngeal mask airway: its role in the difficult airway. Int Anesthesiol Clin 2000; 38: 29-45.
Brain AIJ, Verghese C, Strube PJ. The LMA ‘Proseal’ - a laryngeal mask with an oesophageal vent. Br J Anaesth 2000; 84: 650-4.
Cook TM, Lee G, Nolan JP. The ProSeal laryngeal mask airway: a review of the literature. Can J Anesth 2005; 52: 739-60.
Brimacombe J, Kelle C. The Proseal™ laryngeal mask airway: a randomized, crossover study with the standard laryngeal mask airway in paralyzed, anesthetized patients. Anesthesiology 2000; 93: 104-9.
Natalini G, Franceschetti ME, Pantelidi MT, Rosano A, Lanza G, Bernardini A. Comparison of the standard laryngeal mask airway and the ProSeal laryngeal mask airway in obese patients. Br J Anaesth 2003; 90: 323-6.
Halaseh BK, Sukkar ZF, Hassan LH, Sia AT, Bushnaq WA, Adarbeh H. The use of ProSeal laryngeal mask airway in caesarean section–experience in 3000 cases. Anaesth Intensive Care 2010; 38: 1023-8.
Lim Y, Goel S, Brimacombe JR. The ProSeal laryngeal mask airway is an effective alternative to laryngoscope-guided tracheal intubation for gynaecological laparoscopy. Anaesth Intensive Care 2007; 35: 52-6.
Verghese C, Ramaswamy B. LMA-Supreme™- a new single-use LMA™ with gastric access: a report on its clinical efficacy. Br J Anaesth 2008; 101: 405-10.
Cook TM, Gatward JJ, Handel J, et al. Evaluation of the LMA Supreme™ in 100 non-paralysed patients. Anaesthesia 2009; 64: 555-62.
Timmermann A, Cremer S, Eich C, et al. Prospective clinical and fiberoptic evaluation of the Supreme Laryngeal Mask Airway™. Anesthesiology 2009; 110: 262-5.
Eschertzhuber S, Brimacombe J, Hohlrieder M, Keller C. The Laryngeal Mask Airway Supreme™ - a single use laryngeal mask airway with an oesophageal vent. A randomised, cross-over study with the Laryngeal Mask Airway ProSeal™ in paralysed, anaesthetised patients. Anaesthesia 2009; 64: 79-83.
Hosten T, Gurkan Y, Ozdamar D, Tekin M, Toker K, Solak M. A new supraglottic airway device: LMA-Supreme™, comparison with LMA-Proseal™. Acta Anaethesiol Scand 2009; 53: 852-7.
Seet E, Rajeev S, Firoz T, et al. Safety and efficacy of laryngeal mask airway Supreme versus laryngeal mask airway Proseal™: a randomized controlled trial. Eur J Anaesthesiol 2010; 27: 602-7.
Tham HM, Tan SM, Woon KL, Zhao YD. A comparison of the Supreme laryngeal mask airway with the Proseal laryngeal mask airway in anesthetized paralyzed adult patients: a randomized crossover study. Can J Anesth 2010; 57: 672-8.
Lee AK, Tey JB, Lim Y, Sia AT. Comparison of the single-use LMA supreme with the reusable ProSeal LMA for anaesthesia in gynaecological laparoscopic surgery. Anaesth Intensive Care 2009; 37: 815-9.
Theiler LG, Kleine-Brueggeney M, Kaiser D, et al. Crossover comparison of the Laryngeal Mask Supreme™ and the i-gel™ in simulated difficult airway scenario in anesthetized patients. Anesthesiology 2009; 111: 55-62.
Chew EE, Hashim NH, Wang CY. Randomised comparison of the LMA Supreme with the I-Gel in spontaneously breathing anaesthetised adult patients. Anaesth Intensive Care 2010; 38: 1018-22.
Teoh WH, Lee KM, Suhitharan T, Yahaya Z, Teo MM, Sia AT. Comparison of the LMA Supreme vs the i-gel in paralysed patients undergoing gynaecological laparoscopic surgery with controlled ventilation. Anaesthesia 2010; 65: 1173-9.
Abdi W, Dhonneur G, Amathieu R, et al. LMA Supreme™ versus facemask ventilation performed by novices: a comparative study in morbidly obese patients showing difficult ventilation predictors. Obes Surg 2009; 19: 1624-30.
Abdi W, Amathieu R, Adhoum A, et al. Sparing the larynx during gynecological laparoscopy: a randomized trial comparing the LMA Supreme™ and the ETT. Acta Anaesthesiol Scand 2010; 54: 141-6.
Ali A, Canturk S, Turkmen A, Turgut N, Altan A. Comparison of the laryngeal mask airway SupremeTM and laryngeal mask airway Classic™ in adults. Eur J Anaesthesiol 2009; 26: 1010-4.
van Zundert A, Brimacombe J. The LMA-Supreme™ - a pilot study. Anaesthesia 2008; 63: 202-13.
Lopez AM, Valero R, Brimacombe J. Insertion and use of the LMA Supreme™ in the prone position. Anaesthesia 2010; 65: 154-7.
Sharma V, Verghese C, McKenna PJ. Prospective audit on the use of the LMA-Supreme™ for airway management of adult patients undergoing elective orthopaedic surgery in prone position. Br J Anaesth 2010; 105: 228-32.
Howes BW, Wharton NM, Gibbison B, Cook TM. LMA Supreme™ insertion by novices in manikins and patients. Anaesthesia 2010; 65: 343-7.
Tan BH, Chen EG, Liu EH. An evaluation of the laryngeal mask airway supreme’ in 100 patients. Anaesth Intensive Care 2010; 38: 550-4.
Carron M, Freo U, Ori C. Sensory nerve damage after the use of the LMA Supreme™. Anesthesiology 2010; 112: 1055-6.
Murdoch H, Cook TM. Effective ventilation during CPR via an LMA-Supreme. Anaesthesia 2008; 63: 326.
Braude D, Southard A, Bajema T, Sims E, Martinez J. Rapid sequence airway using the LMA-Supreme as a primary airway for 9 h in a multi-system trauma patient. Resucitation 2010; 81: 1217.
Pearson DM, Young PJ. Use of the LMA-Supreme™ for airway rescue. Anesthesiology 2008; 109: 356-7.
Blair EJ, Mihai R, Cook TM. Tracheal intubation via the Classic™ and Proseal™ laryngeal mask airways: a manikin study using the Aintree Intubating Catheter. Anaesthesia 2007; 62: 385-7.
Allison A, McCrory J. Tracheal placement of a gum elastic bougie using the laryngeal mask airway. Anaesthesia 1990; 45: 419-20.
Greenland KB, Tan H, Edwards M. Intubation via a laryngeal mask airway with an Aintree catheter - not all laryngeal masks are the same. Anaesthesia 2007; 62: 966-7.
Joffe AM, Liew EC. Intubation through the LMA-Supreme™: a pilot study of two techniques in a manikin. Anaesth Intensive Care 2010; 38: 33-8.
Matioc AA. Use of the Arndt airway exchanger catheter set with the Laryngeal Mask Airway Supreme. J Clin Anesth 2009; 21: 152-3.
Mathes AM, Wrobel M, Reus E, Rensing H, Grundmann U. Fiberoptic-guided intubation via the Laryngeal Mask Airway Supreme. J Clin Anesth 2008; 20: 322-3.
Carron M, Freo U, Ori C. Bronchoscope-guided intubation through a Laryngeal Mask Airway Supreme in a patient with a difficult-to-manage airway. J Anesth 2009; 23: 613-5.
Acknowledgement
This study is supported in part by the Department of Anesthesia, Toronto Western Hospital, University of Toronto.
Conflicts of interests
None declared.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author contributions
David T. Wong was responsible for the conception of the review and for writing the manuscript. Jaisy J. Yang helped to accrue articles for the review. Jaisy J. Yang and Narasimhan Jagannathan contributed to both the analysis of the articles and writing the manuscript.
Rights and permissions
About this article
Cite this article
Wong, D.T., Yang, J.J. & Jagannathan, N. Brief review: The LMA Supreme™ supraglottic airway. Can J Anesth/J Can Anesth 59, 483–493 (2012). https://doi.org/10.1007/s12630-012-9673-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-012-9673-0