
Summary
BACKGROUND: Worldwide, drowning is the second leading cause of unintentional death and the leading cause of cardiovascular failure for children [1–3]. The number of near-drownings, where the incident is survived for at least 24 hours, is assumed to be four times as high [5]. In the years 1994 until 2008 there were 44 cases of drowning treated at the children's department of the University of Leipzig. This number shows that even in a medical centre drowning incidents are only occasional incidents. Therefore it is important to know the sequelae and handlings to be able to react in case of an emergency. PATIENTS: A total of 44 children suffering a drowning accident within the last 48 hours who were treated during the period of 01.01.1994 through 30.06.2008 at the Children's Centre at the University of Leipzig. METHODS: A retrospective analysis using a structured questionnaire was done. Social demographic data, accident progress, clinical results and progress as well as outcome of the cases were investigated. RESULTS: During the analysed period in the median three children were treated each year after drowning incidents. Clustering in the summer and winter months and on the weekends was recognizable. The median age was 3.33 years and the group of high risk were children aged 1–3 years, especially boys. Sixty percent of the children came from stable social backgrounds. Half of the children suffered from drowning in created swimming pools or ponds, the rest in natural waters, public pools and sources of water in the household. The median submersion lasted 2 minutes. Correlation of submersions below 1 minute with a good, and submersions above 10 minutes with a negative outcome was shown. A Glasgow Coma Scale (GCS) of 3 points (n = 15) and pupils without light reaction (n = 14) were associated with a lethal outcome or residual neurological deficits. Looking at the laboratory values, correlation between severe acidotic pH-values with a very low base excess, high blood sugar as well as high lactate values and a poor outcome is revealed. Six patients died within the first 24 hours, 6 more over the course suffering organ failure or brain death. Five children retained neurological damages. Twenty-seven children could be released from the clinic healthily. CONCLUSION: The risk of suffering a drowning incident is highest for boys aged 1–3 years, playing in the yard by themselves. Prognosis is depending on multiple factors and especially the circumstances of the accident. High influence is seen in the time of submersion and the need for cardiopulmonary resuscitation. Clinics and laboratory values at the time of hospital admittance may hint to the outcome. Basic life support at the scene of the accident has the highest impact on the outcome. Training of parents and supervisors in prevention and first aid after drowning incidents can avoid accidents.
Zusammenfassung
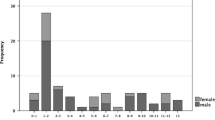
HINTERGRUND: Ertrinken gilt weltweit als die zweithäufigste nicht-natürliche Todesursache bei Kindern sowie als die häufigste Ursache eines Herz-Kreislaufstillstandes im Kindes- und Jugendalter [1–3]. Die Zahl der Fälle von Beinahe-Ertrinken, bei dem der Ertrinkungsunfall mindestens 24 Stunden überlebt wird, wird auf etwa das Vierfache geschätzt [5]. In den Jahren 1994 bis 2008 wurden an der Universitätsklinik für Kinder und Jugendliche Leipzig 44 Patienten nach Ertrinkungsunfall behandelt. Dies zeigt, dass auch in einem Zentrum der Maximalversorgung die Behandlung von Ertrinkungsunfällen nur in Einzelfällen vorkommt. Umso wichtiger ist es, die möglichen Folgen und Handlungsabläufe zu kennen, um im Notfall richtig handeln zu können. PATIENTEN: 44 Kinder mit durchgemachtem Ertrinkungsunfall innerhalb der letzten achtundvierzig Stunden, die im Zeitraum 01.01.1994 bis 30.06.2008 an der Universitätsklinik für Kinder und Jugendliche der Universität Leipzig behandelt wurden. METHODIK: Es erfolgte eine retrospektive Analyse mit einem strukturierten Fragebogen. Soziodemographische Daten, Unfallhergang, erhobene Untersuchungsbefunde sowie klinischer Verlauf und Outcome wurden untersucht. ERGEBNISSE: Im Median wurden 3 Kinder pro Jahr nach Ertrinkungsunfall behandelt. Es ist eine Häufung der Fälle in den Sommer- und den Wintermonaten sowie an den Wochenenden zu erkennen. Der Altersmedian betrug 3,33 Jahre und die Hochrisikogruppe stellten die Ein- bis Dreijährigen, vorzugsweise Jungen, dar. 60 % der Kinder stammten aus stabilen sozialen Verhältnissen. Die Hälfte der Kinder verunglückte an künstlich angelegten Gewässern wie Pools und Gartenteichen, der Rest der Gruppe in natürlichen Gewässern, Schwimmbädern oder Wasserquellen im Haushalt. Die mediane Submersionszeit betrug 2 Minuten. Eine Submersionszeit von unter 1 Minute korrelierte mit einem guten und von über 10 Minuten mit einem schlechten Outcome. Eine Glasgow Coma Scale (GCS) von 3 Punkten (n = 15) sowie lichtstarre Pupillen (n = 14) waren mit einem letalen Ausgang oder dem Zurückbleiben neurologischer Defizite assoziiert. Es ergab sich eine Korrelation zwischen schwer azidotischen pH-Werten mit einem niedrigen Base Excess, hohen Glukose- sowie Laktatwerten und einer negativen Prognose. 6 Patienten verstarben innerhalb der ersten 24 Stunden, 6 weitere im stationären Verlauf durch Organversagen oder Hirntod. 5 Kinder behielten neurologische Folgeschäden zurück. 27 Kinder konnten gesund entlassen werden. SCHLUSSFOLGERUNG: Das höchste Risiko einen Ertrinkungsunfall zu erleiden haben Jungen im Alter zwischen 1 und 3 Jahren, die alleine im Garten spielen. Die Prognose ist von den jeweiligen Unfallumständen abhängig, wobei Submersionszeit und initiale Reanimationspflichtigkeit einen besonderen prädiktiven Aussagewert haben. Klinik und Laborwerte bei Ankunft in der Klinik sind ebenfalls hinweisgebend für das Outcome. Die Erstversorgung am Unfallort ist ausschlaggebend für den Ausgang der Fälle. Schulungen von Eltern und Betreuern zu Prävention und Erster Hilfe bei Ertrinkungsunfällen könnten dazu beitragen Unfälle zu verhindern.
Similar content being viewed by others


Literatur
Brenner RA (2002) Childhood drowning is a global concern – Prevention needs a multifaceted approach. BMJ 324: 1049–50
Idris AH, et al (2003) Recommended Guidelines for Uniform Reporting of Data from Drowning: the "Utstein Style". Circulation 108: 2565–74
WHO Homepage Internet: http://www.who.int/water_sanitation_health/bathing/srwe2full.pdf
CRM: Reisemedizin Spezial: Ertrinken in Deutschland; CRM-Infodienst Reisemedizin aktuell. 2008: 24
Deutsche Lebens-Rettungs-Gesellschaft Internet: http://www.dlrg.de/fileadmin/user_upload/DLRG.de/BAGEH/VortragTh_ner.pdf
Weinstein M, Krieger B (1995) Near-drowning: epidemiology, pathophysilogy and initial treatment. J Emerg Med 14: 461–7
Noble CS (1963) Drowning. Its mechanism and treatment. Canad Med Ass J 89: 402–5
Riede U-N, Schäfer H-E (Hrsg) (2002) Allgemeine und Spezielle Pathologie, 4. aktualisierte Aufl. Georg Thieme Verlag, Stuttgart
Milne S, Cohen A (2006) Secondary drowning in a patient with epilepsy. BMJ 332: 775–6
Hasibeder WR (2003) Drowning. Curr Opin Anaesthesiol 16: 139–46
Hasibeder W (2003) Beinaheertrinken: Epidemiologie – Pathophysiologie – Therapie. Anästhesiol Intensivmed Notfallmed Schmerzth 38: 333–40
Ghofrani H (2004) Lungenödem. Internist 45: 565–72
Hermon M, et al (2003) Monitoring of cerebral oxygen saturation with a jugular bulb catheter after near-drowning and respiratory failure. Wien Klin Wochenschr 115: 128–31
Merz U (2007) Der Ertrinkungsunfall. In: Kiess W, Merkenschlager A, Pfäffle R, Siekmeyer W (Hrsg) Therapie im Kindes- und Jugendalter. Urban und Fischer, S399–404
Pearn J (1985) The management of near drowning. Br Med J 291: 1447–50
Deutsche Lebens-Rettungs-Gesellschaft – Homepage Internet: http://dlrg.de/presse/pm-ertrinkungsstatistik.html
Layon A (2009) Drowning Update 2009. Anesthesiology 110: 1390–401
Hon K-L, et al (2008) Indoor versus outdoor childhood submersion injury in a densly populated city. Acta Paediatr 97: 1261–4
Stadt Leipzig: Bevölkerung Internet: http://www.leipzig.de/de/business/wistandort/zahlen/bevoelkerung/
Graf WD, et al (1995) Predicting outcome in pediatric submersion victims. Ann Emerg Med 26: 312–9
Rimsza M, Schackner RA, Bowen KA, Marshall W (2002) Can child deaths be prevented? The Arizona child fatality review program experience. Pediatrics 110: e11
Levy D, et al (2004) Alcohol involvement in burn, submersion, spinal cord, and brain injuries. Med Sci Monit 10: CR17–24
Grmec S (2009) Comparison of the characteristics and outcome among patients suffering from out-of-hospital primary cardiac arrest and drowning victims in cardiac arrest. Int J Emerg Med 2: 7–12
Claesson A (2008) Characteristics and outcome among patients suffering out-of-hospital cardiac arrest due to drowning. Resuscitation 76: 381–7
Mauritz W, et al (2003) First aid measures by bystanders at the place of accident. A prospective, epidemiologic study in the Vienna area. Wien Klin Wochenschr 115: 698–704
Burghofer K, Köhler M, et al (2008) Erste-Hilfe-Maßnahmen bei Notfällen, Prospektive Beobachtungsstudie bei Primäreinsätzen des RTH Christoph 1. Notfall Rettungsmed 2: 127–36
Marchant J, et al (2008) Bystander basic life support: an important link in the chain of survival for children suffering a drowning or near-drowning episode. Med J Australia 188: 484–5
Eich C (2009) Characteristics of out-of-hospital paediatric emergencies attended by ambulance- and helicopter-based emergency physicians. Resuscitation 80: 888–92
Dahlem P, van Aalderen WM, Bos AP (2007) Pediatric acute lung injury. Paediatr Respir Rev 8: 348–62
Marx M, Golej J, Fürst G, Hermon M, Trittenwein G (1995) Acute respiratory failure (ARDS) in a young child after drowning accident: therapy with exogenous surfactant and high frequency oscillatory ventilation. Wien Klin Wochenschr 107: 146–8
Harries M (2003) Near drowning. BMJ 327: 1336–8
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brüning, C., Siekmeyer, W., Siekmeyer, M. et al. Retrospektive Analyse von 44 Ertrinkungsunfällen von Kindern und Jugendlichen. Wien Klin Wochenschr 122, 405–412 (2010). https://doi.org/10.1007/s00508-010-1400-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-010-1400-7