
Purpose:
To evaluate the feasibility, efficacy, and side effects of dose escalation in hypofractionated stereotactic radiotherapy (hfSRT) for intrapulmonary tumors with the Novalis™ system (BrainLAB AG, Heimstetten, Germany).
Patients and Methods:
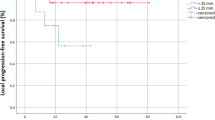
From 07/2003 to 01/2005, 21 patients/39 tumors were treated with 5 × 7 Gy (n = 21; total dose 35 Gy) or 5 × 8 Gy (n = 18; total dose 40 Gy). There were three cases of primary lung cancer, the remainder were metastases. Median gross tumor volume (GTV) and planning target volume (PTV) were 2.89 cm3 (range, 0.15–67.94 cm3) and 25.75 cm3 (range, 7.18–124.04 cm3), respectively.
Results:
Rates of complete remission, partial remission, no change, and progressive disease were 51%, 33%, 3%, and 13%, respectively. No grade 4 toxicity occurred, nearly all patients had grade 1 initially. One grade 3 toxicity, i.e., dyspnea, was documented for a period of 6 months after therapy. Radiosurgery quality assurance guidelines could be met.
Conclusion:
hfSRT of primary and secondary lung tumors using a schedule of five fractions at 7–8 Gy each was well tolerated. Further dose escalation is planned.
Ziel:
Auswertung der Durchführbarkeit, Wirksamkeit und Nebenwirkungen einer Phase-I/II-Studie zur Dosiseskalation bei hypofraktionierter stereotaktischer Radiotherapie (hfSRT) von Lungentumoren mit dem Novalis™-System (BrainLAB AG, Heimstetten).
Patienten und Methodik:
21 Patienten/39 Tumoren wurden von Juli 2003 bis Januar 2005 mit 5 × 7 Gy (n = 21; Gesamtdosis [GD] 35 Gy) oder 5 × 8 Gy (n = 18; GD 40 Gy) bestrahlt. Drei Patienten hatten ein primäres Lungenkarzinom, die übrigen Metastasen. Das mediane „gross tumor volume”(GTV) und Planungszielvolumen (PTV) betrugen 2,89 cm3 (0,15–67,94 cm3) und 25,75 cm3 (7,18–124,04 cm3).
Ergebnisse:
Eine komplette Remission, partielle Remission, keine Änderung und Progression fanden sich bei 51%, 33%, 3% und 13%. Nach initialer Grad-1-Toxizitat in fast allen Fälle trat keine Grad-4-Toxizitat auf. Eine Patientin erlitt eine Grad-3-Toxizität. Die RTOG-Qualitatskriterien für die Radiochirurgie wurden bei allen Patienten erfüllt.
Schlussfolgerung:
Die hfSRT mit 5 × 7 Gy und 5 × 8 Gy wurde gut vertragen. Die Dosiseskalation wird fortgeführt.


Similar content being viewed by others


References
Belderbos J, Heemsbergen W, Hoogeman M, et al. Acute esophageal toxicity in non-small cell lung cancer patients after high-dose conformal radiotherapy. Radiother Oncol 2005;75:157–164.
Belderbos JS, De Jaeger K, Heemsbergen WD, et al. First results of a phase I/II dose escalation trial in non-small cell lung cancer using three-dimensional conformal radiotherapy. Radiother Oncol 2003;66:119–126.
Blomgren H, Lax I, Naslund I, et al. Stereotactic high-dose fraction radiation therapy of extracranial tumors using an accelerator. Clinical experience of the first thirty-one patients. Acta Oncol 1995;34:861–870.
Boda-Heggemann J, Walter C, Mai S, et al. Frameless stereotactic radiosurgery of a solitary liver metastasis using active breathing control and stereotactic ultrasound. Strahlenther Onkol 2006;182:216–221.
Combs SE, Gutwein S, Thilmann C, et al. Reirradiation of recurrent WHO grade III astrocytomas using fractionated stereotactic radiotherapy (FSRT). Strahlenther Onkol 2005;181:768–773.
Downey RJ, Ng K. The management of non-small-cell lung cancer with oligometastases. Chest Surg Clin N Am 2001;11:121–132.
Ernst-Stecken A, Lambrecht U, Ganslandt O, et al. Radiosurgery of small skull-base lesions. No advantage for intensity-modulated stereotactic radiosurgery versus conformal arc technique. Strahlenther Onkol 2005;181:336–344.
Fowler J. Non-standard fractionation in radiotherapy. Int J Radiat Oncol Biol Phys 1984;10:755–759.
Haedinger U, Flentje M, Wulf J, et al. Influence of calculation model on dose distribution in stereotactic radiotherapy for pulmonary targets. Int J Radiat Oncol Biol Phys 2005;61:239–249.
Hall EJ, Brenner D. The radiobiology of radiosurgery: rationale for different treatment regimes for AVMs and malignancies. Int J Radiat Oncol Biol Phys 1993;25:381–385.
Hara R, Kondo T, Aruga T, et al. Stereotactic single high dose irradiation of lung tumors under respiratory gating. Radiother Oncol 2002;63:159–163.
Hellman S, Weichselbaum R. Oligometastases. J Clin Oncol 1995;13:8–10.
Henzel M, Gross M, Hamm K, et al. Stereotactic radiotherapy of meningiomas. Symptomatology, acute and late toxicity. Strahlenther Onkol 2006;182:382–388.
Herfarth KK, Lohr F, Bahner ML, et al. Extracranial stereotactic radiation therapy: set-up accuracy of patients treated for liver metastases. Int J Radiat Oncol Biol Phys 2000;46:329–335.
Hocht S, Stark R, Seiler F, et al. Proton or stereotactic photon irradiation for posterior uveal melanoma? A planning intercomparison. Strahlenther Onkol 2005;181:783–788.
Hof H, Munter M, Hoess A, et al. Stereotactic single-dose radiotherapy of stage I non-small-cell lung cancer (NSCLC). Int J Radiat Oncol Biol Phys 2003;56:335–341.
Koelbl O, Haedinger U, Sauer O, et al. Influence of calculation algorithm on dose distribution in irradiation of non-small cell lung cancer (NSCLC). Collapsed cone versus pencil beam. Strahlenther Onkol 2004;180:783–788.
Krieger T. Monte Carlo- versus pencil-beam-/collapsed-cone-dose calculation in a heterogeneous multi-layer phantom. Phys Med Biol 2005;50:859–868.
Lax I, Blomgren H, Naslund I, et al. Stereotactic radiotherapy of malignancies in the abdomen. Methodological aspects. Acta Oncol 1994;33:677–683.
Lee SW, Park HJ, Ahn SD, et al. Stereotactic body frame based fractionated radiosurgery on consecutive days for primary or metastatic tumors in the lung. Lung Cancer 2003;40:309–315.
Martini N, Burt M, Zakowski MF, et al. Incidence of local recurrence and second primary tumors in resected stage I lung cancer. J Thorac Cardiovasc Surg 1995;109:120–129.
Munter MW, Nill S, Thilmann C, et al. Stereotactic intensity-modulated radiation therapy (IMRT) and inverse treatment planning for advanced pleural mesothelioma. Feasibility and initial results. Strahlenther Onkol 2003;179:535–541.
Nagata Y, Aoki T, Mizowaki T, et al. Clinical outcomes of 3D conformal hypofractionated single high-dose radiotherapy for one or two lung tumors using a stereotactic body frame. Int J Radiat Oncol Biol Phys 2002;52:1041–1046.
Nevinny-Stickel M, Sweeney R, Bale RJ. Reproducibility of patient positioning for fractionated extracranial stereotactic radiotherapy using a double-vacuum technique. Strahlenther Onkol 2004;180:117–122.
Onimaru R, Shimizu S, Kitamura K, et al. Tolerance of organs at risk in small-volume, hypofractionated, image-guided radiotherapy for primary and metastatic lung cancers. Int J Radiat Oncol Biol Phys 2003;56:126–135.
Ruggieri L. Hypofractionation in non-small cell lung cancer (NSCLC): suggestions from modelling both acute and chronic hypoxia. Phys Med Biol 2004;49:4811–4823.
Seegenschmiedt MH. Interdisciplinary documentation of treatment side effects in oncology. Present status and perspectives. Strahlenther Onkol 1998;174:Suppl 3:25–29.
Shaw E, Gillin M, Souhami L, et al. Radiation Therapy Oncology Group: radiosurgery quality assurance guidelines. Int J Radiat Oncol Biol Phys 1993;27:1231–1239.
Sibley GS. Radiotherapy for patients with medically inoperable stage I nonsmall cell lung carcinoma: smaller volumes and higher doses — a review. Cancer 1998;82:433–438.
Sibley GS, Jamieson T, Marks LB, et al. Radiotherapy alone for medically inoperable stage I non-small-cell lung cancer: the Duke experience. Int J Radiat Oncol Biol Phys 1998;40:149–154.
Timmerman R, Papiez L, McGarry R, et al. Extracranial stereotactic radioablation: results of a phase I study in medically inoperable stage I non-small cell lung cancer. Chest 2003;124:1946–1955.
Timmerman R, Papiez L, Suntharalingam M. Extracranial stereotactic radiation delivery: expansion of technology beyond the brain. Technol Cancer Res Treat 2003;2:153–160.
Uematsu M, Shioda A, Tahara K, et al. Focal, high dose, and fractionated modified stereotactic radiation therapy for lung carcinoma patients: a preliminary experience. Cancer 1998;82:1062–1070.
Uematsu M, Shioda A, Suda A, et al. Computed tomography-guided stereotactic radiotherapy for stage I non-small cell lung cancer: a 5-year experience. Int J Radiat Oncol Biol Phys 2001;51:666–670.
Willner J, Baier K, Flentje M. A little to a lot or a lot to a little? An analysis of pneumonitis risk from dose-volume histogram parameters of the lung in patients with lung cancer treated with 3-D conformal radiotherapy. Strahlenther Onkol 2003;179:548–556.
Wulf J, Haedinger U, Oppitz U, et al. Stereotactic radiotherapy of targets in the lung and liver. Strahlenther Onkol 2001;177:645–655.
Yaes RJ, Maruyama Y. On using the linear-quadratic model in daily clinical practice. Int J Radiat Oncol Biol Phys 1991;20:1353–1362.
Zimmermann FB, Geinitz H, Schill S, et al. Stereotactic hypofractionated radiation therapy for stage I non-small cell lung cancer. Lung Cancer 2005;48:107–114.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ernst-Stecken, A., Lambrecht, U., Mueller, R. et al. Hypofractionated Stereotactic Radiotherapy for Primary and Secondary Intrapulmonary Tumors. Strahlenther Onkol 182, 696 (2006). https://doi.org/10.1007/s00066-006-1577-x
Received:
Revised:
DOI: https://doi.org/10.1007/s00066-006-1577-x