
Abstract
Purpose
The purpose of this structured, evidence-based, clinical update was to determine if rapid sequence induction is a safe or effective technique to decrease the risk of aspiration or other complications of airway management.
Source
In June 2006 a structured search of medline from 1966 to present using OVID software was undertaken with the assistance of a reference librarian. Medical subject headings and text words describing rapid sequence induction or intubation (RSI), crash induction or intubation, cricoid pressure and emergency airway intubation were employed. OVID’s therapy (sensitivity) algorithm was used to maximize the detection of randomized trials while excluding non-randomized research. The bibliographies of eligible publications were hand-searched to identify trials not identified in the electronic search.
Principal findings
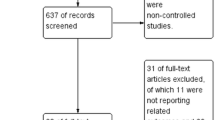
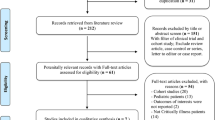
A total of 184 clinical trials were identified of which 163 were randomized controlled trials (RCTs). Of these clinical trials, 126 evaluated different drug regimens with 114 being RCTs. Only 21 clinical trials evaluated non-pharmacologic aspects of the RSI with 18 RCTs identified. A parallel search found 52 trials evaluating cricoid pressure (outside of the context of an RSI technique) with 44 classified as RCTs. Definitive outcomes such as prevention of aspiration and mortality benefit could not be evaluated from the trials. Likewise, the impact on adverse outcomes of the different components of RSI could not be ascertained.
Conclusion
An absence of evidence from RCTs suggests that the decision to use RSI during management can neither be supported nor discouraged on the basis of quality evidence.
Résumé
Objectif
Cette mise à jour clinique structurée, basée sur des données probantes, avait pour objectif de déterminer si l’induction en séquence rapide est une technique sécuritaire ou efficace pour réduire le risque d’inhalation ou d’autres complications de prise en charge des voies respiratoires.
Source
Une recherche structurée de MEDLINE, allant de 1966 à nos jours, à l’aide du logiciel OVID, a été entreprise en juin 2006 avec l’assistance d’un bibliothécaire documentaliste. Les titres de sujets et les termes de textes médicaux décrivant l’induction ou l’intubation en séquence rapide (RSI), la «crash induction» ou intubation, la pression cricox00CF:dienne et l’intubation des voies respiratoires en urgence ont été utilisés. L’algorithme de thérapie (sensibilité) d’OVID a servi à maximiser la détection d’études randomisées tout en excluant les recherches non randomisées. Les bibliographies des publications admissibles ont été cherchées manuellement pour identifier les études qui n’avaient pas été relevées par la recherche électronique.
Constatations principales
Au total, 184 études cliniques ont été identifiées, desquelles 163 étaient des études randomisées contrôlées (RCT). De ces études cliniques, 126 ont évalué différents régimes médicamenteux, 114 étant des RCT. Seules 21 études cliniques ont évalué des aspects non pharmacologiques de l’induction en séquence rapide, dont 18 étaient des RCT. Une recherche parallèle a mis en évidence 52 études évaluant la pression cricoÏdienne (hors du contexte d’une technique de RSI), dont 44 étaient classées comme RCT. Des pronostics définitifs, tels que la prévention d’une inhalation et les bienfaits par rapport à la mortalité, n’ont pas pu être évalués à partir des études. De même, l’impact sur les devenirs indésirables des différentes composantes de la RSI n’a pas pu être déterminé.
Conclusion
Un manque de données probantes issues de RCT suggère que la décision d’utiliser la RSI pendant la prise en charge d’un patient ne peut être ni recommandée ni déconseillée sur la base de données probantes de qualité.
Article PDF
Similar content being viewed by others

References
Brimacombe JR, Berry AM. Cricoid pressure. Can J Anaesth 1997; 44:414–25.
Morton HJ, Wylie WD. Anaesthetic deaths due to regurgitation or vomiting. Anaesthesia 1951; 6:190–201,205.
Woodbridge PD.“Crash induction„for tracheal intubation. JAMA 1967; 202:845.
Warner MA, Warner ME, Weber JG. Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology 1993; 78:56–62.
Mellin-Olsen J, Fasting S, Gisvold SE. Routine preoperative gastric emptying is seldom indicated. A study of 85,594 anaesthetics with special focus on aspiration pneumonia. Acta Anaesthesiol Scand 1996; 40:1184–8.
Olsson GL, Hallen Hambraeus-Jonzon Aspiration during anaesthesia: a computer-aided study of 185,358 anaesthetics. Acta Anaesthesiol Scand 1986; 30:84–92.
Kluger MT, Short TG. Aspiration during anaesthesia: a review of 133 cases from the Australian Anaesthetic Incident Monitoring Study (AIMS). Anaesthesia 1999; 54:19–26.
Warner MA, Warner ME, Warner DO, Warner LO, Warner EJ. Perioperative pulmonary aspiration in infants and children. Anesthesiology 1999; 90:66- 71.
Mort TC. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: a justification for incorporating the ASA guidelines in the remote location. J Clin Anesth 2004; 16:508–16.
Lockey DJ, Coats T, Parr MJ. Aspiration in severe trauma: a prospective study. Anaesthesia 1999; 54:1097–8.
Hardoff R, Sula M, Tamir A, et al. Gastric emptying time and gastric motility in patients with Parkinson’s disease. Mov Disord 2001; 16:1041–7.
Heyland DK, Tougas G, King D, Cook DJ. Impaired gastric emptying in mechanically ventilated, critically ill patients. Intensive Care Med 1996; 22:1339–44.
Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obstet Gynecol 1946; 52:191–205.
Dronen SC, Merigian KS, Hedges JR, Hoekstra JW, Borron SW. A comparison of blind nasotracheal and succinylcholine-assisted intubation in the poisoned patient. Ann Emerg Med 1987; 16:650–2.
Sagarin MJ, Barton ED, Chng YM, Walls RM National Emergency Airway Registry Investigators. Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts. Ann Emerg Med 2005; 46:328–36.
Sakles JC, Laurin EG, Rantapaa AA, Panacek EA.Airway management in the emergency department: a one-year study of 610 tracheal intubations. Ann Emerg Med 1998; 31:325–32.
Bair AE, Filbin MR, Kulkarni RG, Walls RM. The failed intubation attempt in the emergency department: analysis of prevalence, rescue techniques, and personnel. J Emerg Med 2002; 23:131–40.
Li J, Murphy-Lavoie H, Bugas Martinez J, Preston C. Complications of emergency intubation with and without paralysis. Am J Emerg Med 1999; 17:141–3.
Rose WD, Anderson LD, Edmond SA. Analysis of intubations. Before and after establishment of a rapid sequence intubation protocol for air medical use. Air Med J 1994; 13:475–8.
Pearson S. Comparison of intubation attempts and completion times before and after the initiation of a rapid sequence intubation protocol in an air medical transport program. Air Med J 2003; 22:28–33.
Ma OJ, Atchley RB, Hatley R, Green M, Young J, Brady W. Intubation success rates improve for an air medical program after implementing the use of neuromuscular blocking agents. Am J Emerg Med 1998; 16:125–7.
Davis DP, Stern J, Sise MJ, Hoyt DB. A follow-up analysis of factors associated with head-injury mortality after paramedic rapid sequence intubation. J Trauma 2005; 59:486–90.
Falcone RE, Herron H, Dean Werman H.Emergency scene endotracheal intubation before and after the introduction of a rapid sequence induction protocol. Air Med J 1996; 15:163–7.
Ochs M, Davis D, Hoyt D, Bailey D, Marshall L, Rosen P. Paramedic-performed rapid sequence intubation of patients with severe head injuries. Ann Emerg Med 2002; 40:159–67.
Wang HE, Yealy DM. Out-of-hospital rapid sequence intubation: is this the“success„we envisioned? Ann Emerg Med 2002; 40:168–71.
Benumof JL. Preoxygenation: best method for both efficacy and efficiency. Anesthesiology 1999; 91:603–5.
Drummond GB, Park GR. Arterial oxygen saturation before intubation of the trachea. An assessment of oxygenation techniques. Br J Anaesth 1984; 56:987–93.
Kashyap L, Yaddanapudi LN, Sandhya. Arterial desaturation during induction with and without preoxygenation: evaluation of four techniques. Anaesth Intensive Care 1993; 21:811–3.
Gold MI, Duarte I, Muravchick S. Arterial oxygena- tion in conscious patients after 5 minutes and after 30 seconds of oxygen breathing. Anesth Analg 1981; 60:313–5.
Goldberg ME, Norris MC, Larijani GE, Marr AT, Seltzer JL. Preoxygenation in the morbidly obese: a comparison of two techniques. Anesth Analg 1989; 68:520–2.
Norris MC, Dewan DM. Preoxygenation for cesarean section: a comparison of two techniques. Anesthesiology 1985; 62:827–9.
Chiron B, Laffon M, Ferrandiere M, Pittet JF, Marret H, Mercier C. Standard preoxygenation technique versus two rapid techniques in pregnant patients. Int J Obstet Anesth 2004; 13:11–4.
Baraka AS, Taha SK, Aouad MT, EI-Khatib MF, Kawkabani NI. Preoxygenation: comparison of maximal breathing and tidal volume breathing techniques. Anesthesiology 1999; 91:612–6.
Gambee AM, Hertzka RE, Fisher DM. Preoxygenation techniques: comparison of three minutes and four breaths. Anesth Analg 1987; 66:468–70.
Valentine SJ, Marjot R, Monk CR. Preoxygenation in the elderly: a comparison of the four-maximal breath and three-minute techniques. Anesth Analg 1990; 71:516–9.
McCarthy G, Elliott P, Mirakhur RK, McLoughlin C A comparison of different pre-oxygenation techniques in the elderly. Anaesthesia 1991; 46:824–7.
Baraka AS, Taha SK, El-Khatib MF, Massouh FM, Jabbour DG, Alameddine MM. Oxygenation using tidal volume breathing after maximal exhalation. Anesth Analg 2003; 97:1533–5.
Baraka A, Haroun-Bizri S, Khoury S, Chebab IR.Single vital capacity breath for preoxygenation. Can J Anesth 2000; 47:1144–6.
Dixon BJ, Dixon JB, Carden JR, et al. Preoxygenation is more effective in the 25 degrees head-up position than in the supine position in severely obese patients: a randomized controlled study. Anesthesiology 2005: 102:1110–5.
Altermatt FR, Munoz HR, Delfino AE, Cortinez LI.Pre-oxygenation in the obese patient: effects of posture on tolerance to apnoea. Br J Anaesth 2005; 95:706–9.
Cotton BR, Smith G. The lower oesophageal sphincter and anaesthesia. Br J Anaesth 1984; 56:37–46.
Vanner RG, Pryle BJ, O’Dwyer JP, Reynolds F. Upper oesophageal sphincter pressure and the intravenous induction of anaesthesia. Anaesthesia 1992; 47:371–5.
Tayal VS, Riggs RW, Marx JA, Tomaszewski CA, Schneider RE. Rapid-sequence intubation at an emergency medicine residency: success rate and adverse events during a two-year period. Acad Emerg Med 1999; 6:31–7.
Dufour DG, Larose DL, Clement SC. Rapid sequence intubation in the emergency department. J Emerg Med 1995; 13:705–10.
Sivilotti ML, Ducharme J. Randomized, double-blind study on sedatives and hemodynamics during rapid-sequence intubation in the emergency department: The SHRED Study. Ann Emerg Med 1998; 31:313–24.
Morris J, Cook TM. Rapid sequence induction: a national survey of practice. Anaesthesia 2001; 56:1090–7.
Sivilotti ML, Filbin MR, Murray HE, Slasor P, Walls RM; NEAR Investigators. Does the sedative agent facilitate emergency rapid sequence intubation?Acad Emerg Med 2003; 10:612–20.
Reynolds SF, Heffner J. Airway management of the critically ill patient: rapid-sequence intubation. Chest 2005; 127:1397–1412.
Oglesby A. Should etomidate be the induction agent of choice for rapid sequence intubation in the emergency department? Emerg Med J 2004; 21:655–9.
Zed PJ, Abu-Laban RB, Harrison DW. Intubating conditions and hemodynamic effects of etomidate for rapid sequence intubation in the emergency department: an observational cohort study. Acad Emerg Med 2006; 13:378–83.
Smith DC, Bergen JM, Smithline H, Kirschner R. A trial of etomidate for rapid sequence intubation in the emergency department. J Emerg Med 2000; 18:13–6.
Skinner HJ, Biswas A, Mahajan RP. Evaluation of intubating conditions with rocuronium and either propofol or etomidate for rapid sequence induction. Anaesthesia 1998; 53:702–6.
Lindgren L, Yli-Hankala A, Randell T, Kirvela M, Scheinin M, Neuvonen PJ. Haemodynamic and cat- echolamine responses to induction of anaesthesia and tracheal intubation: comparison between propofol and thiopentone. Br J Anaesth 1993; 70:306–10.
Wilmot G, Bhimsan N, Rocke DA, Murray WB.Intubating conditions and haemodynamic changes following thiopentone or propofol for early tracheal intubation. Can J Anaesth 1993; 40:201–5.
Vohra A, Thomas AN, Harper NJ, Pollard BJ. Non- invasive measurement of cardiac output during induction of anaesthesia and tracheal intubation: thiopentone and propofol compared. Br J Anaesth 1991; 67:64–8.
Sagarin MJ, Chiang V, Sakles JC, et al. Rapid sequence intubation for pediatric emergency airway management. Pediatr Emerg Care 2002; 18:417–23.
Sokolove Price DD, Okada P. The safety of e tomi date for emergency rapid sequence intubation of pediatric patients. Pediatr Emerg Care 2000; 16:18–21.
Fellows IW, Yeoman PM, Selby C, Byrne AJ. The effect of anaesthetic induction with etomidate on the endocrine response to surgical trauma. Eur J Anaesthesiol 1985; 2:285–90.
Jackson WL Jr. Should we use etomidate as an induction agent for endotracheal intubation in patients with septic shock? A critical appraisal. Chest 2005; 127:1031–8.
Schenarts CL, Burton JH, Riker RR. Adrenocortical dysfunction following etomidate induction in emergency department patients. Acad Emerg Med 2001; 8:1–7.
Weiss-Bloom LJ, Reich DL. Haemodynamic responses to tracheal intubation following etomidate and fen- tanyl for anaesthetic induction. Can J Anaesth 1992; 39:780–5.
Brossy MJ, James MF, Janicki PK. Haemodynamic and catecholamine changes after induction of anaesthesia with either thiopentone or propofol with suxametho- nium. Br J Anaesth 1994; 72:596–8.
Reves JG, Fragen RJ, Vinik HR, Greenblatt DJ.Midazolam: pharmacology and uses. Anesthesiology 1985; 62:310–24.
Lavazais S, Debaene B. Choice of the hypnotic and the opioid for rapid-sequence induction. Eur J Anaesthesiol Suppl 2001; 23:66–70.
McCollum JS, Dundee JW. Comparison of induction characteristics of four intravenous anaesthetic agents. Anaesthesia 1986; 41:995–1000.
Wong AK, Teoh GS. Intubation without muscle relaxant: an alternative technique for rapid tracheal intubation. Anaesth Intensive Care 1996; 24:224–30.
Dobson AP, McCluskey A, Meakin G, Baker RD.Effective time to satisfactory intubation conditions after administration of rocuronium in adults. Comparison of propofol and thiopentone for rapid sequence induction of anaesthesia. Anaesthesia 1999; 54:172–6.
McKeating K, Bali IM, Dundee JW. The effects of thiopentone and propofol on upper airway integrity. Anaesthesia 1988; 43:638–40.
Perry JJ, Lee J, Wells G. Are intubation conditions using rocuronium equivalent to those using succinylcholine? Acad Emerg Med 2002; 9:813–23.
Erhan E, Ugur G, Alper I, Gunusen I, Ozyar B.Tracheal intubation without muscle relaxants: remifentanil or alfentanil in combination with propofol. Eur J Anaesthesiol 2003; 20:37–43.
Hans P, Brichant JF, Hubert B, Dewandre PY, Lamy M. Influence of induction of anaesthesia on intubat- ing conditions one minute after rocuronium administration: comparison of ketamine and thiopentone. Anaesthesia 1999; 54:276–9.
Sparr HJ, Giesinger S, Ulmer H, Hollenstein-Zacke M, Luger TJ. Influence of induction technique on intu- bating conditions after rocuronium in adults: comparison with rapid-sequence induction using thiopentone and suxamethonium. Br J Anaesth 1996; 77:339–42.
Naguib M, Samarkandi AH, El-Din ME, Abdullah K, Khaled M, Alharby SW. The dose of succinylcholine required for excellent endotracheal intubating conditions. Anesth Analg 2006; 102:151–5.
Naguib M, Samarkandi A, Riad W, Alharby SW. Optimal dose of succinylcholine revisited. Anesthesiology 2003; 99:1045–9.
Kopman AF, Zhak B, Lai KS. The“intubating dose„of succinylcholine: the effect of decreasing doses on recovery time. Anesthesiology 2003; 99:1050–4.
EI-Orbany MI, Joseph NJ, Salem R, Klowden AJ. The neuromuscular effects and tracheal intubation conditions after small doses of succinylcholine. Anesth Analg 2004; 98:1680–5.
Benumof JL, Dagg R, Benumoff R. Critical hemoglobin desaturation will occur before return to an unparalyzed state following 1mg/kg intravenous succinylcholine. Anesthesiology 1997; 87:979–82.
Hardman JG, Wills JS, Aitkenhead AR. Factors determining the onset and course of hypoxemia during apnea: an investigation using physiological modelling. Anesth Analg 2000; 90:619–24.
Heier T, Feiner JR, Lin J, Brown R, Caldwell JE.Hemoglobin desaturation after succinylcholine-indu- ced apnea: a study of the recovery of spontaneous ventilation in healthy volunteers. Anesthesiology 2001; 94:754–9.
Hayes AH, Breslin DS, Mirakhur RK, Reid JE, O’Hare RA. Frequency of haemoglobin desaturation with the use of succinylcholine during rapid sequence induction of anaesthesia. Acta Anaesthesiol Scand 2001; 45:746–9.
Naguib M, Samarkandi AH, Abdullah K, Riad W, Alharby SW. Succinylcholine dosage and apnea- induced hemoglobin desaturation in patients. Anesthesiology 2005; 102:35–40.
Sluga M, Ummenhofer W, Studer W, Siegemund M, Marsch SC. Rocuronium versus succinylcholine for rapid sequence induction of anesthesia and endotracheal intubation: a prospective, randomized trial in emergent cases. Anesth Analg 2005; 101:1356–61.
Harris CE, Murray AM, Anderson JM, Grounds RM, Morgan M. Effects of thiopentone, etomidate and propofol on the haemodynamic response to tracheal intubation. Anaesthesia1988; 43 (Suppl):32–6.
Hug CCJr. Does opioid ` anesthesia’ exist?Anesthesiology1990; 73:1–4.
Lev R, Rosen P. Prophylactic lidocaine use preintuba- tion: a review. J Emerg Med 1994; 12:499–506.
Brucia JJ, Owen DC, Rudy The effects of lido- caine on intracranial hypertension. J Neurosci Nurs 1992; 24:205–14.
Robinson N, Clancy M. In patients with head injury undergoing rapid sequence intubation, does pretreat- ment with intravenous lignocaine/lidocaine lead to an improved neurological outcome? A review of the literature. Emerg Med J 2001; 18:453–7.
Feng CK, Chan KH, Liu KN, Or CH, Lee comparison of lidocaine, fentanyl, and esmolol for attenuation of cardiovascular response to laryngos- copy and tracheal intubation. Acta Anaesthesiol Sin 1996; 34:61–7.
Lin PL, Wang YP, chou»™ Chan HL, Huang HH.Lack of intravenous lidocaine effects on HRV changes of tracheal intubation during induction of general anesthesia. Acta Anaesthesiol Sin 2001; 39:77–82.
Chraemmer-Jorgensen B, Hoilund-Carlsen PF, Marving J, Christensen V. Lack of effect of intravenous lidocaine on hemodynamic responses to rapid sequence induction of general anesthesia: a double-blind controlled clinical trial. Anesth Analg 1986; 65:1037–41.
Butler J, Jackson R. Best evidence topic report. Lignocaine as a pretreatment to rapid sequence intubation in patients with status asthmaticus. Emerg Med J 2005; 22:732.
Butler J, Jackson R. Towards evidence based emergency medicine: best BETs from Manchester Royal Infirmary. Lignocaine premedication before rapid sequence induction in head injuries. Emerg Med J 2002; 19:554.
Helfman SM, Gold MI, DeLisser EA, Herrington CA. Which drug prevents tachycardia and hypertension associated with tracheal intubation: lidocaine, fentanyl, or esmolol? Anesth Analg 1991; 72:482–6.
Singh H, Vichitvejpaisal P, Gaines GY, White PF.Comparative effects of lidocaine, esmolol, and nitro- glycerin in modifying the hemodynamic response to laryngoscopy and intubation. J Clin Anesth 1995; 7:5–8.
Poulton TJ, James FM 3rd. Cough suppression by lidocaine. Anesthesiology 1979; 50:470–2.
Yukioka H, Yoshimoto N, Nishimura K, Fujimori M.Intravenous lidocaine as a suppressant of coughing during tracheal intubation. Anesth Analg 1985; 64:1189–92.
Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults. A prospective investigation of 297 tracheal intubations. Anesthesiology 1995; 82:367–76.
Vanner RG, Asai T. Safe use of cricoid pressure. Anaesthesia 1999; 54:1–3.
Jackson SH. Efficacy and safety of cricoid pressure needs scientific validation. Anesthesiology 1996; 84:751–2.
Kron SS. Questionable effectiveness of cricoid pressure in preventing aspiration (Letter). Anesthesiology 1995; 83:431.
Schwartz DE, Cohen NH. Questionable effectiveness of cricoid pressure in preventing aspiration (Letter, reply). Anesthesiology 1995; 83:432.
Vanner RG, Pryle BJ. Nasogastric tubes and cricoid pressure. Anaesthesia 1993; 48:1112–3.
Smith KJ, Ladak S, Choi PT, Dobranowski J. The cricoid cartilage and the esophagus are not aligned in close to half of adult patients. Can J Anesth 2002; 49:503–7.
Smith KJ, Dobranowski J, Yip G, Dauphin A, Choi PT.Cricoid pressure displaces the esophagus: an observational study using magnetic resonance imaging. Anesthesiology 2003; 99:60–4.
Allman KG. The effect of cricoid pressure on airway patency. J Clin Anesth 1995; 7:197–9.
Moynihan RJ, Brock-Utne JG, Archer JH, Feld LH, Kreitzmand TR. The effect of cricoid pressure on preventing gastric insufflation in infants and children. Anesthesiology 1993; 78:652–6.
Vanner RG. Tolerance of cricoid pressure by conscious volunteers. Int J Obstet Anesth 1992; 1:195–8.
Lawes EG, Duncan PW, Bland B, Gemmel L, Downing JW. The cricoid yoke - a device for providing consistent and reproducible cricoid pressure. Br J Anaesth 1986; 58:925–31.
Hartsilver EL, Vanner RG. Airway obstruction with cricoid pressure. Anaesthesia 2000; 55:208–11.
Aoyama K, Takenaka I, Sata T, Shigematsu A.Cricoid pressure impedes positioning and ventilation through the laryngeal mask airway. Can J Anaesth 1996; 43:1035–40.
MacG Palmer JH, Ball DR. The effect of cricoid pressure on the cricoid cartilage and vocal cords: an endoscopic study in anaesthetised patients. Anaesthesia 2000; 55:263–7.
Hodgson RE, Gopalan PD, Burrows RC, Zuma K.Effect of cricoid pressure on the success of endotracheal intubation with a lightwand. Anesthesiology 2001; 94:259–62.
Shulman GB, Connelly NR. A comparison of the Bullard laryngoscope versus the flexible fiberoptic bronchoscope during intubation in patients afforded inline stabilization. J Clin Anesth 2001; 13:182–5.
Wood PR. Direct laryngoscopy and cervical spine stabilisation. Anaesthesia 1994; 49:77–8.
Turgeon AF, Nicole PC, Trepanier CA, Marcoux S, Lessard MR. Cricoid pressure does not increase the rate of failed intubation by direct laryngoscopy in adults. Anesthesiology 2005; 102:315–9.
Mort TC.Preoxygenation in critically ill patients requiring emergency tracheal intubation. Crit Care Med 2005; 33:2672–5.
Lawes EG, Campbell I, Mercer D. Inflation pressure, gastric insufflation and rapid sequence induction. Br J Anaesth 1987; 59:315–8.
Ruben H, Krudsen EJ, Carugati G. Gastric inflation in relation to airway pressure. Acta Anaesthesiol Scand 1961; 5:107–14.
Petito SP, Russell WJ. The prevention of gastric insufflation - a neglected benefit of cricoid pressure. Anaesth Intensive Care 1988; 16:139–43.
Author information
Authors and Affiliations
Corresponding author
Additional information
No funding was provided and no conflict of interests.
This work was supported by the Departments of Anesthesiology at The Ottawa Hospital and the University of Ottawa. The authors declare no commercial or non-commercial affiliations that are or may be perceived to be a conflict of interest with the work, and any other associations such as consultancies.
Rights and permissions
About this article
Cite this article
Neilipovitz, D.T., Crosby, E.T. No evidence for decreased incidence of aspiration after rapid sequence induction. Can J Anesth 54, 748–764 (2007). https://doi.org/10.1007/BF03026872
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03026872